

English sweating sickness (sudor anglicus) was a mysterious, highly virulent epidemic disease that struck England five times between 1485 and 1551. Characterized by sudden onset, profuse drenching sweat, and an exceptionally rapid mortality rate, it remains one of medical history’s greatest unsolved puzzles.
English sweating sickness, also called English sweat or sudor anglicus, is a mysterious, highly virulent epidemic disease that appeared in England five times between 1485 and 1551, characterized by sudden onset, profuse sweating, high fever, and rapid death (often within 24 hours). The disease has disappeared completely since 1551 and remains one of medicine’s greatest unsolved mysteries.

Historical facts are
| Aspect | Details |
| Outbreaks | 1485, 1508, 1517, 1528, 1551 (five major epidemics) |
| Duration per outbreak | Only a few weeks in any locality |
| Geographic spread | Mostly England; 1528-1529 spread to Hamburg, Scandinavia, Poland, Russia, and the Netherlands. |
| Did Not spread to | France, Italy (except Calais) |
| Mortality | Very high, especially in 1485, 1517, and 1528; more severe among rich than poor. |
| Primary source | Dr. John Caius’s 1552 account, A Boke or Counseill Against the Disease. |
What Caused the English Sweating Sickness?
The exact cause remains unknown. Modern hypotheses include the following:
| Proposed Cause | Evidence | Limitations |
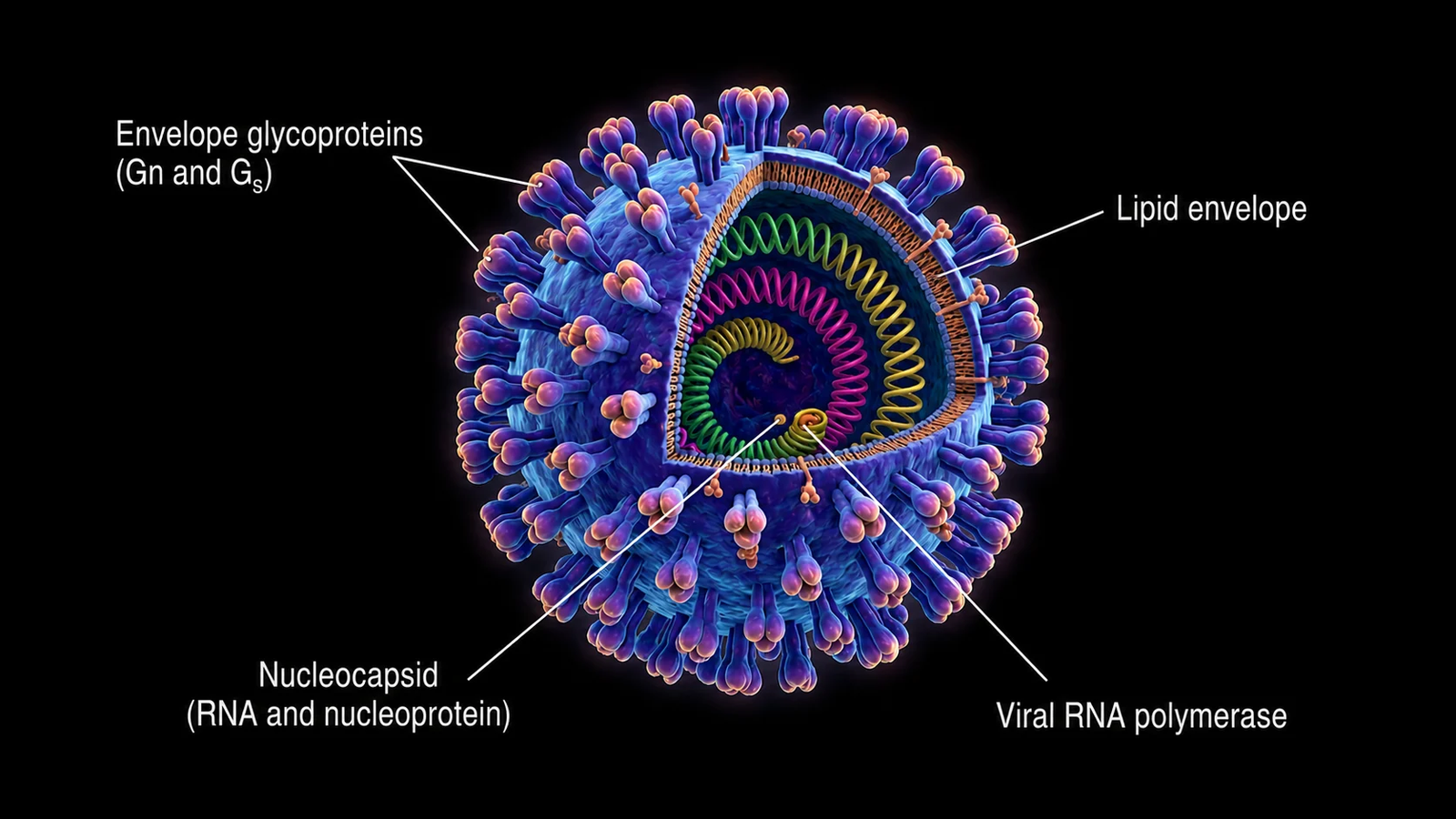
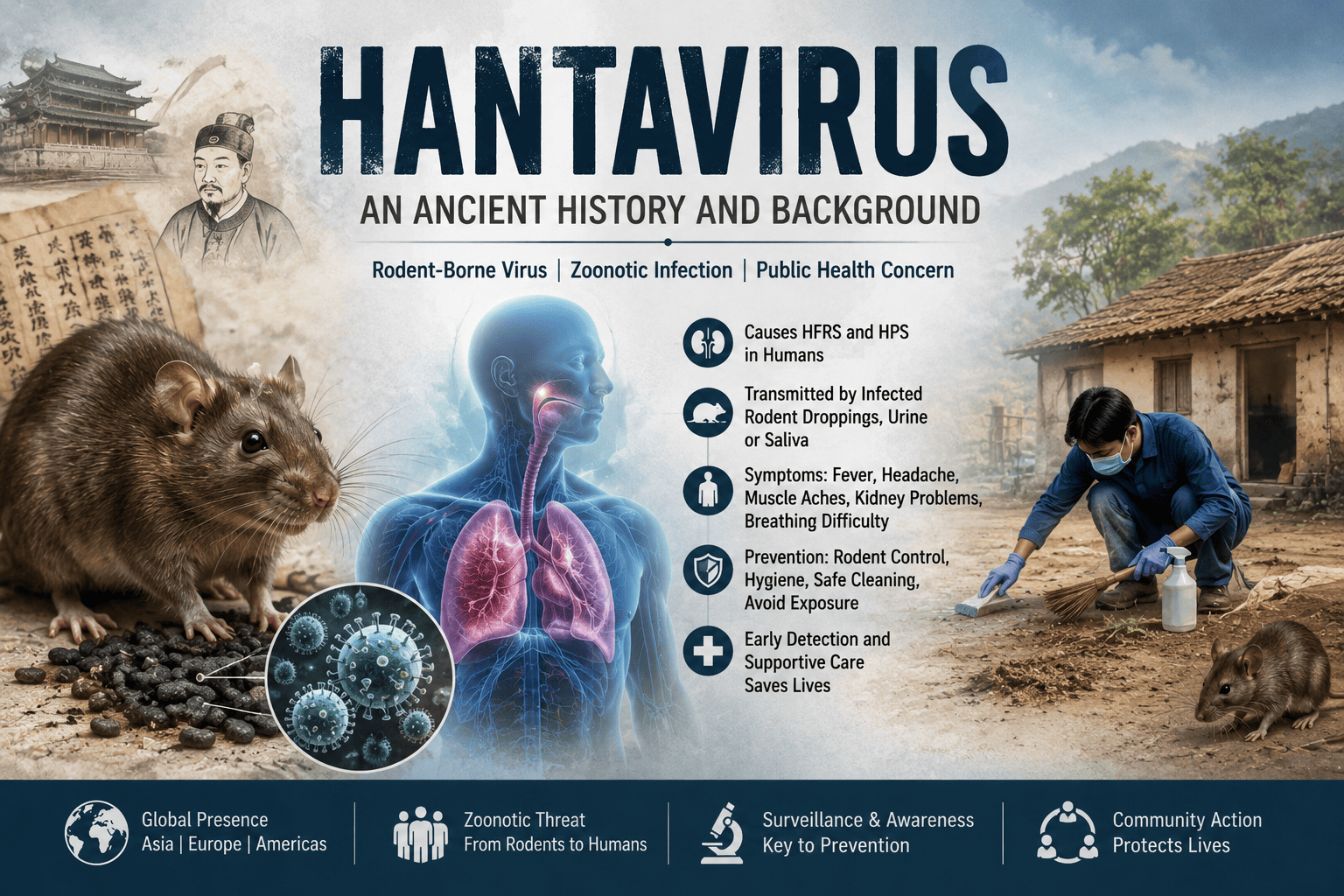
| Hantavirus infection | Most favored by contemporary scholars and actively documented in emerging pathogen research by the National Institutes of Health, it matches rapid onset, sweating, and high mortality. | No direct evidence; genetic proof impossible. |
| Relapsing fever (Lice/tick-borne) | Many symptoms; possible vector-borne mechanism | Doesn’t fully explain all characteristics |
| Mosquito-borne viral diseases like dengue | Seasonal pattern (late spring/summer); vector susceptible to climate change | Dengue lasts >24 hours; usually has rash (not mentioned by Caisus) |
| Anthrax | Proposed by some researchers | Inconsistent with clinical picture |
| Influenza or typhus | —– | Unlikely based on the symptom profile |
Contributing factors suggested
- Dirt and filth (Caius’s original theory)
- Insect vectors (all epidemics occurred in late spring/summer)
- Climate change affecting vector populations.
Types / Related Diseases:
| Disease | Time period | Key Differences |
| English sweating sickness | 1485 to 1551 | No rash (usually ); very high mortality; confined to England mostly). |
| Picardy sweat | 1718 to 1861 (france) | Always had rash lasting ~1 week; lower mortality; resembles English sweat |
| Other epidemic fevers | various | Different clinical presentation; not true “sweating sickness” |
Some researchers suggest hantavirus infection explains both English sweating sickness and Picardy sweat.
What Were the Symptoms of English Sweating Sickness?
Stage 1—Initial (0.5 to 3 hours);
- Sudden apprehension/anxiety
- Violent cold shivers/rigors
- Giddiness/dizziness
- Severe headache
- Exhaustion/prostration
- Severe pains in neck, shoulders, and limbs
Stage 2—Sweating (1 to 3 hours after onset):
- Violent, drenching sweating (sudden onset)
- Sense of intense heat
- Severe headache worsens
- Delirium
- Rapid pulse (tachycardia)
- Intense thirst
Stage 3—The Final Phase
- “ Marvellous heaviness and desire to sleep” (extreme heaviness, drowsiness)
- Death may occur 3 to 18 hours after onset
- If the patient survives 24 hours, recovery is usually complete.
- Occasionally: vesicular rash (rare)
Key distinguishing features
- Extraordinarily rapid course (death within 24 hours)
- Profuse sweating is a hallmark.
- Young, healthy people were frequent victims (unusual for most diseases)
- No immunity after infection; multiple attacks possible.
How Was the Sweating Sickness Diagnosed?
Important caveat: The disease no longer exists, so modern diagnosis is not applicable. The historical diagnosis was clinical:
| Method | Historical Context |
| Clinical recognition | Based on sudden onset + profuse sweating + rapid progression |
| Differentiation from plague | Sweating and rapid course distinguished it from the plague. |
| Differentiation from other fevers | Unique sweating pattern and < 24 hours’ course |
| No laboratory tests | No microbiology existed in 1485 to 1551 |
Modern retrospective diagnosis
- Cannot be confirmed definitively
- Diagnosis based on historical records and symptoms descriptions
- No surviving pathogen to test
Prevention Measures (Historical Context)
Since the disease disappeared, modern prevention is not applicable. Historical recommendations from Caius:
- Maintain cleanliness (avoid dirt and filth)
- Avoid Contact with infected persons
- Stay indoors during outbreaks
- Avoid travelling to affected areas
- Flee early if outbreak beings
Modern implications (if caused by a vector-borne pathogen)
- Vector control (mosquitos, ticks, lice)
- Avoid insect bites
- Environmental sanitation
Control Measures (Historical)
- Isolation: Separate sick individuals from healthy population
- Quarantine: Restrict movement during outbreaks
- Fleeing: Wealthy people often fled to the countryside.
- Environmental cleanup: Remove filth and stagnant water
- Outbreak containment: Each epidemic lasted only weeks naturally
No specific treatment existed then or now (disease is extinct).
Historical supportive care
- Bed rest in cool environment
- Fluid replacement (though limited options)
- Comfort measures for pain and fever
- Moral support (disease caused extreme apprehension)
Modern approach (if disease reappeared)
- Aggressive fluid and electrolyte management
- Oxygen therapy if respiratory distress
- Hemodynamic support for shock
- ICU care for critical patients
- No antiviral would be available initially
What Was the Prognosis and Mortality Rate?
- If survived 24 hours, → usually complete recovery.
- Death typically occurred 3 to 18 hours after symptom onset.
Public Health Awareness
Historical awareness
- Caused extreme fear among population
- Rich more affected than poor (unusual pattern)
- People knew to flee early if outbreak occurred
- John Caius’s book becomes primary public health guidance.
Modern relevance
- Important historical lesson about emerging infectious diseases.
- Shows how disease can appear and disappear mysteriously
- Emphasizes need for rapid response to novel pathogens
- Illustrates importance of detailed clinical documentation
Community Engagement
Historical community response
- Mass panic during outbreaks
- Community flight to avoid infection
- Religious processions and prayers for protection
- Local quarantine enforcement.
Modern community engagement for similar emerging diseases:
- Rapid risk communication
- Community isolation support
- Contact tracing infrastructure
- Mental health support for fear/anxiety
IEC Materials
If this were a modern emerging disease:
Posters:
- “Sudden fever + profuse sweating = medical emergency”
- “Don’t wait—seek care within hours.”
- “Avoid contact with sick persons.”
Leaflets:
- Symptoms recognition guide
- When to seek medical help
- Prevention measures (vector control if applicable)
Training materials:
- For healthcare workers on rapid recognition
- Isolation protocols
- Case management guidelines
Social media:
- Quick symptom checklists
- Emergency hotline numbers
- MYth-busting about transmission
Historical IEC:
- John Caius’s printed book (1552) was the first major public health pamphlet on the disease.
Role of Public Health Department
Historical role, limited in the 15th to 16th century
- Local authorities enforced quarantine
- Burial regulations during outbreaks
- Travel restrictions between towns
Modern Public Health Role for Similar Emerging Diseases
- Surveillance: Early detection of unusual febrile illness clusters.
- Laboratory capacity: Rapid pathogen identification
- Outbreak investigation: Identify source and transmission pattern
- Risk communication: Accurate, timely public information
- Isolation facilities : Quarantine infected individuals
- Contact tracing: Identify and monitor exposed persons
- International notification: WHO reporting if needed.
Magnitude of the disease
- Total outbreaks: 5 major epidemics, e.g., 1485, 1508, 1517, 1528, 1551
- First outbreak (1485): Killed several thousand within couple months
- 1502 outbreak: Possibly killed Arthur, prince of Wales (Henry VIII’s brother)
- Mortality rate: Very high; some estimates 30% to 50% in severe outbreaks
- 1528-29 European outbreak: Swept through eastern Europe with high mortality
- Duration: Each outbreak lasted only weeks in any locality.
Risk Factors
- Season: Late spring or summer; all epidemics occurred then
- Age/Health: Young, healthy people frequently victimized (unusual)
- Social class: More severe among rich than poor
- Geography: England mostly; 1528 spread to Europe
- No immunity: Previous infection did not confer immunity
- Multiple attacks: The same person could be infected several times.
Global Risks
Current risk: zero—the disease has been extinct since 1578
Hypothetical risks if pathogen reappeared
- No immunity in modern population
- No Specific treatment or vaccine available
- Rapid spread before detection (very fast progression)
- High mortality if similar to historical outbreaks
- Global health emergency potential due to novel pathogen
Why Did the Sweating Sickness Mysteriously Disappear?
- The pathogen may have mutated to lower virulence
- Vector disappeared or changed behavior
- Host reservoir eliminated
- Climate change affected transmission
- Unknown factors are the most likely explanation
Current Status
English sweating sickness is EXTINCT—no cases since 1551 and no similar disease since 1578. The Picardy sweat in France (1718 to 1861) was similar but had a consistent rash and lower mortality. Modern scholars continue to debate the exact cause, but the disease remains one of medical history’s greatest mysteries.
Why English Sweating Sickness Was Unique:
- Rapid death: 3 to 18 hours from onset, faster than Plague
- Profuse sweating: Hallmark symptoms not seen in other epidemics
- Victim profile: Young, healthy, wealthy people affected mostly.
- Mystery cause: Still unknown after 500+ years
- Completely disappeared: No similar disease since 1578
- Seasonal: Only late spring/summer outbreaks
- No immunity: Repeated infections common
- Geographic: Mostly confined to England
This disease remains a critical case study in emerging infectious diseases and demonstrates how pathogens can emerge, devastate populations, and then mysteriously vanish.