
The Bombay blood group, also known as the hh or Oh phenotype, is a rare blood type characterized by the complete absence of the H antigen on red blood cells. First discovered in Mumbai/Bombay, India, in 1952 by Dr. Y.M. Bhende, it occurs in about one in 10,000 people in India and is even rarer globally at roughly 0.0004%. It is extremely rare worldwide but more prevalent in India due to genetic factors like consanguinity.
Discovery and Rarity of the Bombay Blood Group
It derives its name from its initial identification among relatives in Mumbai. The condition is most prevalent in South Asia, including India, Pakistan, and Iran, due to the inheritance of two recessive hh alleles from the FUT1 gene on the chromosome.
Genetic Basis of the Bombay Blood Group
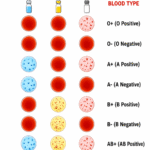
The H antigen, produced by the dominant H gene (FUT1), serves as the precursor for A and B antigens in the ABO system. In HH individuals, both FUT1 alleles are inactive, preventing H antigen formation and thus blocking A or B expression, regardless of ABO genotype. Red blood cells of this group lack A, B, and H antigens but contain anti-A, anti-B, and anti-H antibodies in serum. This makes it phenotypically resemble group O but with critical differences in antigen profile.
Clinical Implication
Transfusion challenges arise as hh blood reacts against all standard ABO types (including O), requiring donor blood from another hh individual, often a relative. Organ transplants also demand HH-compatible donors, though recent cases like kidney transplants in India have succeeded.
| Aspect | Bombay hh Compatibility |
| Donate To | Only Bombay (hh) |
| Receive From | Only bombay (hh) |
| Risk with Others | Fatal hemolysis from anti-H |
Global Prevalence
It occurs in about 0.0004% of the world’s population, or roughly one in 250,000 to one million people globally, with the highest rates in South Asia, Taiwan (1 in 8,000), and pockets of the Middle East. In Europe and populations of European descent, it’s as low as one in 1,000,000.
Differences Between ABO and Rh Incompatibility
ABO and Rh incompatibilities both cause hemolytic disease in newborns (HDN) due to maternal antibodies attacking fetal red blood cells, but they differ in antigens, severity, and management.
Antigens
ABO involves A/B antigens with naturally occurring IgM/IgG antibodies (common in O mothers vs. A/B fetuses); Rh targets the D antigen, requiring prior sensitization to form IgG anti-D.
Severity
ABO is milder, often causing jaundice or anemia in first pregnancies without hydrops fetalis; Rh is severe, risking fetal loss, hepatosplenomegaly, or kernicterus in subsequent pregnancies.
Differences
| Aspect | ABO Incompatibility | Rh Incompatibility |
| Common Scenario | Mother O, Fetus A/B | Mother Rh⁻, fetus Rh⁺ |
| Antibody Type | Pre-existing IgM/IgG | IgG after sensitization |
| First Pregnancy Affected | Yes, often mild | Rarely (needs prior exposure) |
| Coombs Test | Weekly positive direct | Strongly positive direct/indirect |
| Prevention | Rarely needed | RhoGAM at 28 weeks/postpartum. |
Artificial Blood
Artificial blood, also called blood substitutes or oxygen therapeutics, mimics red blood cells’ oxygen-carrying function without fully replicating whole blood clotting or immune roles.
What Is Artificial Blood?
It includes hemoglobin-based oxygen carriers (HBOCs) from modified animal/human hemoglobin and perfluorocarbons (PFCs) that dissolve gases, used to temporarily boost oxygen delivery in low-blood states.
Uses:
- Emergency trauma or surgery with heavy blood loss.
- Remote areas lacking donor blood.
- Enhancing chemotherapy oxygen to tumors or aiding in sickle cell crises.
Advantages of Artificial Blood
As of 2026, artificial blood research focuses on lab-grown red blood cells (RBCs) from stem cells and synthetic oxygen carriers (AOCs), driven by donor shortages and emergencies.
These substituents offer universal compatibility without blood typing, eliminating mismatch risks, and are pathogen-free, reducing HIV and hepatitis transmission. They have long shelf lives (over a year vs. 1 month for donor blood), no refrigeration needs, and immediate usability in emergencies or remote areas.
Stem Cell-derived RBCs
In July 2025, University of Konstanz and Queen Mary University researchers discovered the CXCL12 chemokine triggers nucleus expulsion in erythroblasts, boosting artificial RBC production efficiency from reprogrammed stem cells for scalable blood manufacturing.
Synthetic Oxygen Carriers
Perftoran (PFC-based AOC) remains approved in Russia and others, with over 35,000 uses; U.S. military funds ErythroMer, a hemoglobin polymer in preclinical trials for trauma without refrigeration. Clinical trials in the UK and Japan test AOCs for trauma, with the New York Blood Center advancing toward viable options. Lyophilized platelets and stem cell “blood pharming” for rare types progress, alongside polyhemoglobin for ischemia reduction, though no new global approvals yet.
Disadvantages of Artificial Blood
HBOCs can cause vasoconstriction, hypertension, and higher mortality in trials due to nitric oxide scavenging; many products like HemAssist failed Phase III. PFCs need emulsions, may trigger flu-like symptoms, thrombocytopenia, or immune phagocytosis, and deliver limited oxygen without supplements. High costs, short circulation (20 to 30 hours), and lack of clotting/immunity functions limit them to temporary use; none are FDA-approved for routine transfusion.
Role in Cancer Therapy
Artificial blood shows promise in enhancing cancer survival by addressing tumor hypoxia—low oxygen levels that shield tumors from radiotherapy and chemotherapy—potentially improving treatment efficacy and patient lifespan. Research highlights oxygen-carrying substitutes like hemoglobin-based oxygen carriers (HBOCs) and perfluorocarbons (PFCs) that boost tumor oxygenation, sensitizing hypoxic cancer cells to therapies and possibly extending survival in solid tumors. A 2025 review emphasizes artificial blood’s potential to overcome transfusion limitations (e.g., shortages, immunosuppression risks) for cancer patients needing frequent RBCs, aiding anemia management without promoting progression seen in donor blood.
Survival Impact
No, large human trials confirm direct survival extension yet, but preclinical data suggest better outcomes via enhanced drug/radiation penetration; end-of-life transfusions yield ~ 1 month mean survival, hinting substitutes could match or exceed this safely. Current uses focus on supportive care in advanced cancer, with ongoing trials for trauma potentially extending to oncology.
Natural VS. Artificial Blood
Natural blood always has antigens determining its groups, e.g., A, B, AB, or O, even if rare or untyped. Blood without groups cannot be natural; it aligns with artificial substituents developed to avoid typing, reduce shortages, and enable immediate use. As of 2025-2026, synthetic blood shows promise for emergencies but isn’t a full human blood replacement yet. Trials confirm no blood group requirement, confirming such blood is artificial by design.