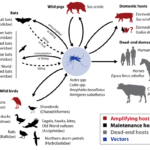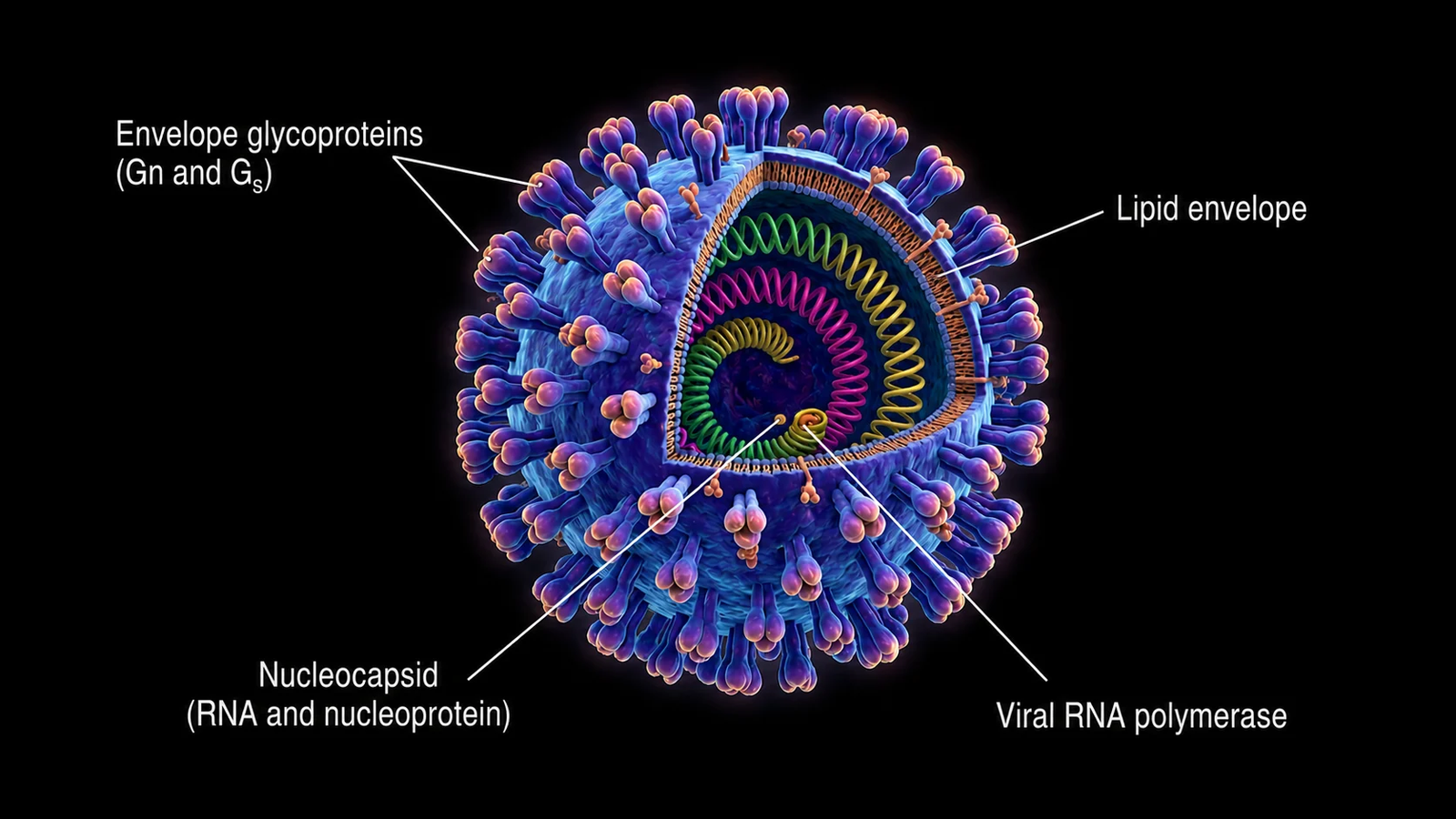
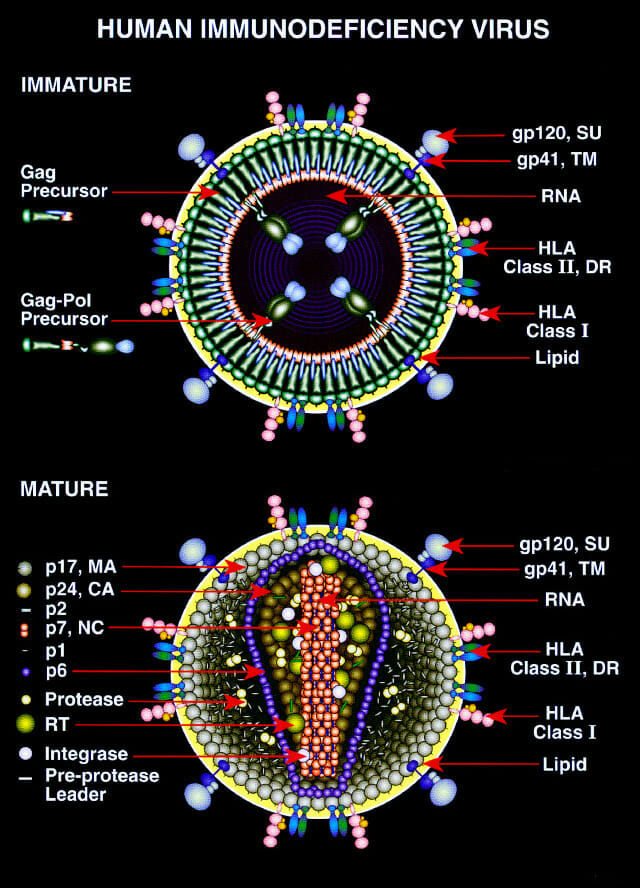


Def:- JEV is an enveloped, single-stranded, positive-sense RNA virus that belongs to the genus Flavivirus (group-B arbovirus) within the family Flaviviridae. It is primarily transmitted to humans by the infective bite of Culex Vishnoi group mosquitoes, with pigs, horses, and water birds acting as important reservoir hosts.
JEV causes inflammation of the brain (encephalitis) and is the leading cause of viral encephalitis in Asia & the Western Pacific. Humans are “dead-end hosts”; they do not contribute to further transmission because viremia remains low & transient. There is only one serotype of JEV, but considerable genetic variability exists, classified into five genotypes based on the sequence of the viral envelope gene. A man develops the disease after 5-15 days of being bitten by an infected mosquito. Man is an incidental “dead end” host.
Japanese encephalitis has a long and complex history spanning thousands of years. Its clinical recognition occurred much more recently. Molecular analysis suggests that JEV originated around 3000 years ago and gradually spread across Asia. The first clearly recorded clinical case of JEV was documented in Japan in 1871. Major outbreaks in Japan followed, most notably in 1924 when over 6,000 cases were reported, with further epidemics in 1927, 1934, & 1935. The initial isolation of the virus from human brain tissue occurred in 1924, though it was not definitively identified as JEV until a decade later through experiments in monkey brains. JEV is now recognized as a major mosquito-borne disease with a well-documented history from the 20th century onward, according to phylogenetic & ecological evidence.
Magnitude of the Problem of JEV in India
Japanese encephalitis is a significant public health problem in India. The first evidence of the presence of the JE virus was in 1952, with the first case reported in 1955 in Tamil Nadu. Since then, JE outbreaks have been reported from different parts of the country. During the recent past (1998-2019), about 24 states & union territories have reported JE incidence. As of mid-2025, JE cases have been reported in 11 states across India. JE remains endemic in around 355 districts of 24 states/UTs overall. Uttar Pradesh being a hotspot responsible for over 75% of cases in some years. Now Assam is bearing a significant burden of JE. JE predominantly affects children under 15 years and rural populations involved in agriculture, causing neurological complications or death. Major outbreaks have occurred in states like West Bengal, Uttar Pradesh (notably Gorakhpur), Assam, Bihar, Odisha, and Northeast India. Vaccination programs started in 2006 & expanded under the universal immunization program in 2011. Yet JE continues to cause sporadic outbreaks, with a shifting age pattern seen in some regions. Surveillance & control efforts include vaccination and vector control, but the disease burden remains high in many endemic districts, particularly during monsoon and post-monsoon seasons when transmission peaks.
Current high-risk states in India
In 2025 (till September), nearly 600 cases of JE were reported across affected states, with deaths ranging up to 79 in the same period. In 2024 nearly 1472 cases of JE were reported, and 1107 cases in 2023. High-risk states with consistently higher JE cases include Assam, Uttar Pradesh, West Bengal, Bihar, Tamil Nadu, Kerala, Karnataka, Jharkhand, Odisha, Manipur, Meghalaya, and Nagaland, among others. Assam alone accounts for about 30%-50% of total JE cases in recent years (2025), marking it as a critical focus area for control efforts. Other historically endemic states include Andhra Pradesh, Haryana, Goa, and parts of north and northeast India.
Show recent JE case trends by state & year
Here are recent trends in Japanese encephalitis cases by state & year in India from 2018 to 2025 (till Sept.).
| State | 2018 | 2019 | 2020 | 2021 | 2022 | 2023 | 2024 | 2025 |
|---|---|---|---|---|---|---|---|---|
| Assam | 509 | 642 | 320 | 218 | 456 | 525 | 670 | 389 |
| Bihar | 74 | 135 | 29 | 38 | 24 | 70 | 51 | 12 |
| Jharkhand | 66 | 112 | 44 | 180 | 86 | 52 | 114 | 18 |
| Manipur | 57 | 343 | 29 | 13 | 66 | 64 | 44 | 13 |
| Meghalaya | 90 | 191 | 38 | 2 | 69 | 89 | 132 | 45 |
| West bengal | 140 | 82 | 41 | 47 | 54 | 37 | 31 | 7 |
| Uttar Pradesh | 323 | 235 | 100 | 153 | 124 | 92 | 61 | 21 |
| Tamil Nadu | 147 | 231 | 47 | 37 | 28 | 20 | 47 | 31 |
| Maharashtra | 6 | 35 | 3 | 0 | 2 | 5 | 5 | 2 |
| Odisha | 143 | 195 | 14 | 18 | 31 | 29 | 22 | 15 |
This pattern highlights persistent JE endemicity in northeastern, eastern, and northern India, reinforcing the need for ongoing surveillance, vaccination, and vector control.