
Herpes simplex virus (HSV) is a common, contagious virus from the herpesviridae family that causes lifelong infections, primarily oral or genital sores.
Definition
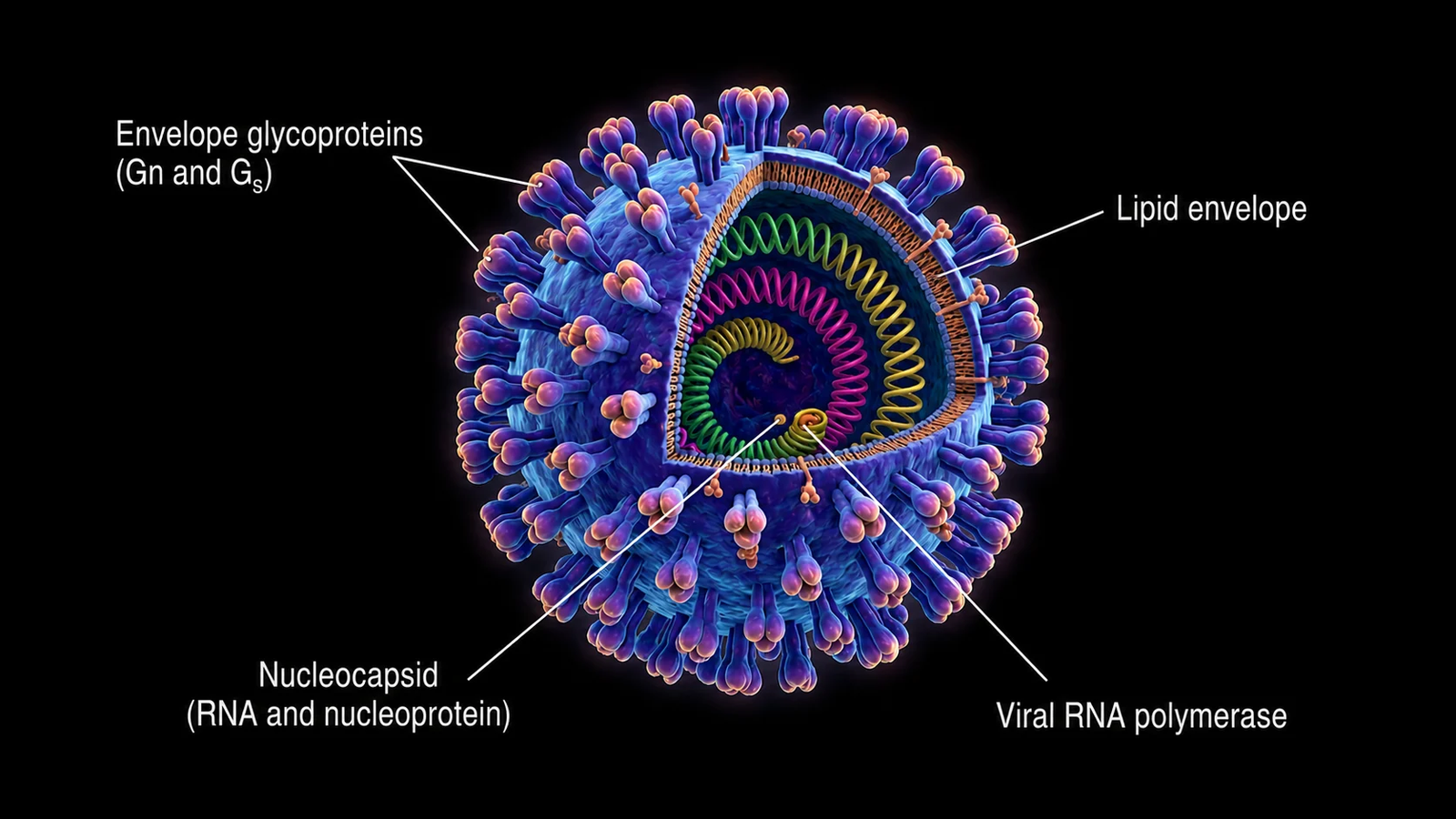
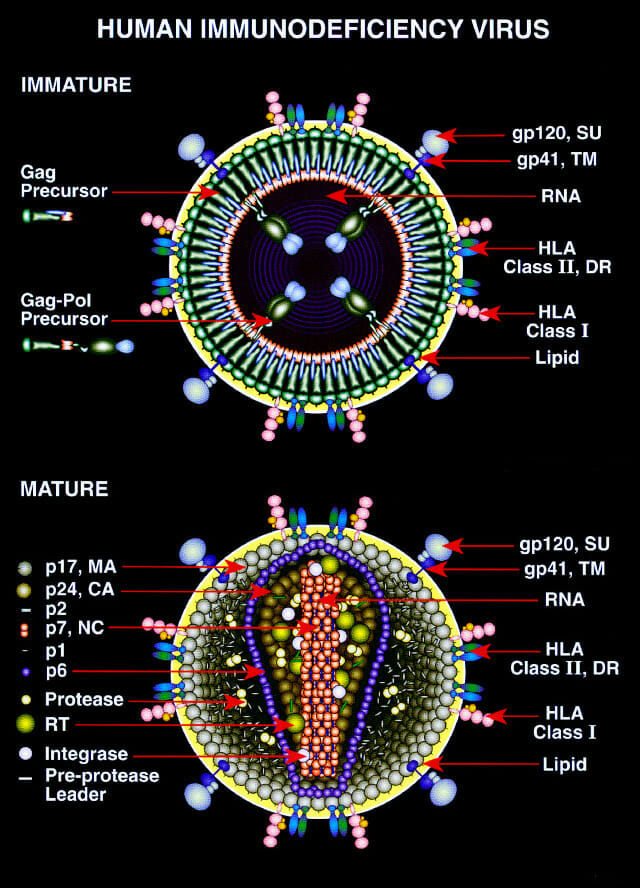
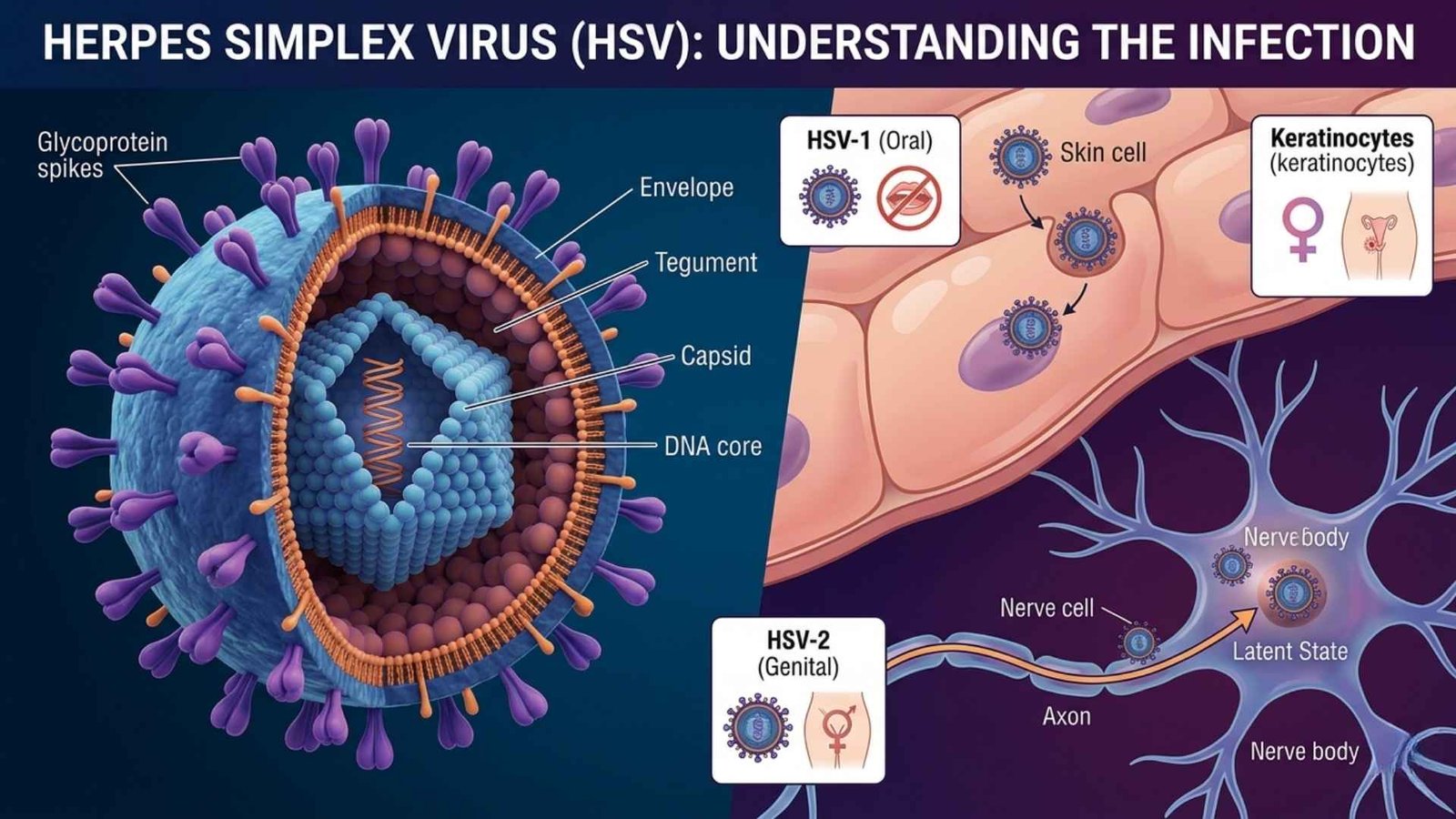
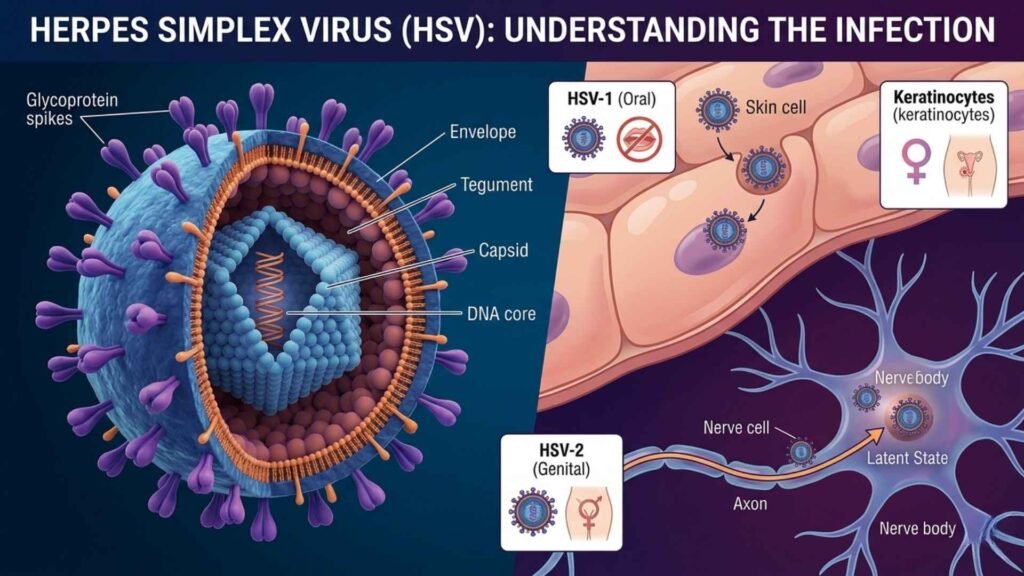
HSV is a double-stranded DNA virus that infects humans, establishing latency in nerve cells after initial infection and reactivating periodically.
Causes
It spreads via direct skin-to-skin contact, including kissing, oral sex, or genital contact with infected secretions, even without visible symptoms due to asymptomatic shedding.
Main Types
HSV-1
HSV-1 typically causes oral herpes (cold sores on the mouth/lips) but can infect genitals.
HSV-2
HSV-2 mainly causes genital herpes but can affect the mouth.
Symptoms
Painful blisters or ulcers form, crust over, and heal; initial outbreaks may include fever, swollen glands, and flu-like symptoms. Many infections are asymptomatic.
Diagnosis
A clinical exam identifies typical sores; confirmation uses lab tests.
Diagnostic Methods
A PCR swab test detects viral DNA (most accurate).
Viral culture from blisters.
Blood tests for antibodies (IgM for recent, IgG for past infection).
Prevention Measures
Use condoms/dental dams, avoid contact during outbreaks, and disclose status to partners. No vaccine exists.
Control Measures
Antiviral therapy suppresses outbreaks and reduces transmission; contact tracing for partners is also important.
Treatment
Antivirals like acyclovir, valacyclovir, or famciclovir shorten outbreaks and prevent recurrences; they are not curative.
Latest Antiviral Treatment for Herpes Outbreaks
Standard antiviral treatments like acyclovir, valacyclovir, and famciclovir remain first-line for herpes outbreaks, taken episodically or daily for suppression. These nucleoside analogs inhibit viral DNA replication, shortening outbreaks by 1–2 days if started early and reducing transmission by 50% with daily use.
Emerging Treatments
Pritelivir (a helicase-primase inhibitor) succeeded in phase 3 (2025) for immunocompromised patients with refractory HSV, showing superior lesion healing over standard care; FDA filing is expected in 2026.
ABI-5366 from Assembly Bio reduced HSV-2 shedding by 94% in phase Ib (2025), advancing to phase II mid-2026 with weekly/monthly dosing potential. No major new approvals for general outbreaks as of March 2026; consult providers for off-label or trial access.
Vaccines
HSV-1 and HSV-2 cannot be cured by vaccine, as the virus establishes lifelong latency in nerve cells after infection, with no treatments eliminating it completely. Antiviral drugs like acyclovir manage symptoms and reduce outbreaks/transmission but do not eradicate the virus.
No approved vaccines exist as of March 2026 to prevent or treat HSV-1 and HSV-2. Several candidates (e.g., Moderna’s mRNA therapeutic and BioNTech’s preventive) are in clinical trials, but none have succeeded yet. Gene editing eliminated 90% of HSV-1 in preclinical mouse models, with reduced shedding, but human trials are pending. Other research, like ABI-5366, focuses on suppression, not cure.
Public Awareness
Education reduces stigma; campaigns emphasize asymptomatic spread and testing importance.
Community Engagement
Support groups and counseling help manage emotional impact and promote safe practices.
IEC Materials
Information, education, and communication tools include brochures, posters, and videos on symptoms, prevention, and stigma reduction.
Role of Public Health Department
Surveillance, antiviral access programs, awareness campaigns, and STI clinic integration.
Magnitude
HSV infects over half the global population.
Global Burden
HSV-1 affects 3.7 billion people under 50 (67%).
HSV-2 affects 491 million aged 15 to 49 (13%), causing 5.3 million new genital cases yearly.
Indian Burden
India has high HSV-2 seroprevalence (10% to 40% in adults); urban STI clinics report frequent cases, though national data is limited.
Differences Between HSV-1 and HSV-2 in Transmission and Symptoms
HSV-1 and HSV-2 are the two main types of herpes simplex virus, differing primarily in typical transmission routes and symptom locations, though overlap exists.
Transmission Differences
HSV-1 spreads mainly through nonsexual contact like kissing or sharing utensils via saliva or skin around the mouth; it can also be transmitted genitally via oral sex.
HSV-2 transmits primarily through sexual contact like vaginal, anal, or oral with genital or anal areas, though both spread asymptomatically via skin-to-skin contact.
Symptom Differences
| Aspect | HSV-1 | HSV-2 |
|---|---|---|
| Primary Site | Oral (cold sores on lips/mouth) | Genital (sores on genitals, buttocks, thighs) |
| Outbreak Frequency | Less frequent recurrences | More frequent and severe recurrences |
| Initial symptoms | Tingling, blisters around the mouth, milder flu-like effects | Painful genital ulcers, fever, swollen glands; often more intensive first outbreak |
Both cause itching, blisters that crust over, and possible asymptomatic shedding, but HSV-2 genital outbreaks tend to be more painful and recurrent.
How are HSV-1 and HSV-2 diagnosed and tested?
HSV-1 and HSV-2 are diagnosed through a combination of clinical evaluation and lab tests that detect the virus or antibodies, with methods varying by symptom presence.
Clinical Diagnosis
Providers first examine sores or lesions for characteristic appearances like blisters or ulcers. This guides testing but isn’t definitive alone, as symptoms mimic other conditions.
Swab-Based Tests
PCR (Polymerase Chain Reaction)
Gold standard; swabs from active sores detect HSV DNA, distinguishing HSV-1 from HSV-2 with high accuracy (fastest, most sensitive).
Viral Culture
Grows virus from swabbed sore cells in lab; specific but less sensitive, especially if taken late in outbreak (50% to 75% accuracy).
Blood Tests
Type-Specific Antibody Tests (IgG/IgM)
Detect antibodies in blood; IgM suggests a recent infection, and IgG indicates past exposure.
ELISA or Western Blot differentiates HSV-1/HSV-2 via glycoproteins gG-1/gG-2 (useful without sores but can’t prove outbreak site).
Western blot is most accurate for serology but costly and slow.
Key Consideration
PCR from sores is preferred during outbreaks; blood tests are for asymptomatic screening.
No routine screening is recommended for low-risk individuals; results take hours (PCR) to days (culture).
Common Complications of HSV Infection
HSV infections are generally mild but can lead to several complications, especially in vulnerable groups like newborns or immunocompromised individuals or during primary outbreaks.
Common Complication
Recurrent outbreaks: Frequent flare-ups cause ongoing pain, distress, and reduced quality of life.
Secondary bacterial infections: Open sores become infected, leading to cellulitis or worsened healing.
Neurological issues: Aseptic meningitis (8% of cases), encephalitis (brain inflammation), or sacral nerve dysfunction causing urinary retention and constipation.
Severe or Rare Issues
| Complication | Description | Risk groups |
|---|---|---|
| Neonatal herpes | Life-threatening disseminated infection from mother to baby during birth | Newborns |
| Ocular herpes (keratitis) | Eye sores leading to vision loss or blindness | HSV-1 carriers |
| Increased HIV Risk | Genital sores facilitate HIV transmission | Those with STIs |
| Eczema herpeticum | Widespread skin infection | Atopic dermatitis patients |
Immunocompromised patients face heightened risks like esophagitis, pneumonia, or myelitis.