How Does Trichomoniasis Increase HIV Transmission Risk
How does Trichomoniasis increase HIV transmission risk :-
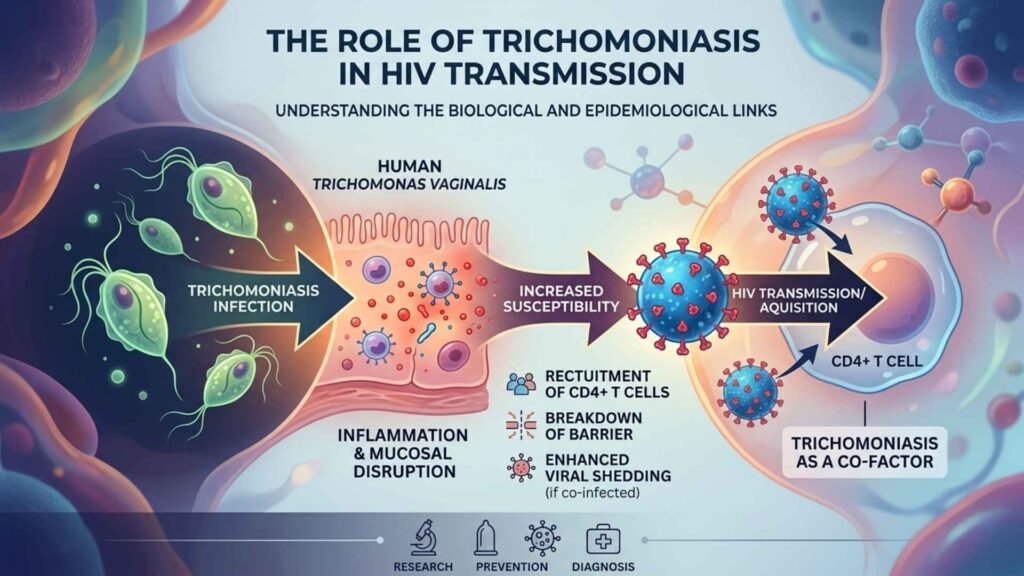
Trichomoniasis heightens HIV transmission risk by causing genital inflammation and mucosal damage, creating easier entry points for the virus during sexual contact. Studies quantify this as roughly a 1.5-fold increase in HIV acquisition odds.
Biological Mechanisms
The parasite induces inflammation, drawing HIV-susceptible immune cells like CD4 +T cells to the genital tract and causing micro-tears or bleeding that breach natural barriers. In HIV-positive individuals, it boosts local viral shedding, amplifying infectiousness.
Supporting Evidence
Meta-analysis show infected people face 50% higher HIV acquisition risk HR 1.5, 95% CI 1.3 to 1.7 with stronger effects in high-prevalence regions. Treating trichomoniasis can thus lower HIV incidence.
B) How to Treat Trichomoniasis to Reduce HIV-Risk
Treating trichomoniasis effectively clears the parasite and reduces associated HIV transmission risk by alleviating genital inflammation and viral shedding. Standard antibiotic regimens, especially multidose for high-risk groups, achieve high cure rates and lower HIV susceptibility.
Recommended Treatments
Primary options include metronidazole 2 gram as a single oral dose or 500mg twice daily for 7 days, or Tinidazole 2gram single dose, the 7 days course is preferred for women, pregnant individuals, or those with HIV to boost cure rates above 90%. Partners must receive simultaneous treatment to prevent reinfection, with abstinence from sex for 7 days post-treatment.
HIV-Risk Reduction
Successful treatment in HIV-positive women cuts genital HIV viral load e.g. by 0.5 log10 copies, curbing transmission to partners; studies show it halves HIV shedding beyond ART effects alone. For HIV-negatives, it restores mucosal barriers, dropping acquisition risk by addressing the 1.5-fold elevation from active infection. Follow-up testing at 3 months ensures clearance.
C) How Effective is Metronidazole in Treating Trichomoniasis
Metronidazole is highly effective for treating trichomoniasis, with cure rates typically ranging from 84% to 98% using recommended regimens. It remains the first-line antibiotic, outperforming alternatives in some multi-dose scenarios.
Single Dose Regimen
A 2 gram oral dose achieves 84% to 98% cure rates but higher failure risk about 1.87 times vs. multi-dose, due to reinfection or resistance. It’s convenient for compliance but less ideal for HIV-positive patients or recurrent cases.
Multi-Dose Regimen
500mg twice daily for 7 days boosts cure rates (halves re-positive tests at 1 month) and is preferred for women, pregnant individuals, or high-risk groups, reaching over 95% efficacy. Partners should be treated simultaneously to prevent ping-pong reinfection.
Factors Affecting Efficacy
Resistance is emerging up to 10% breakthrough, linked to non-compliance or single dosing: tinidazole offers similar or better results 92% to 100% with fewer failures. Follow-up testing at 3 months confirms clearance.
D) Trichomoniasis Differences in Men and Women Symptoms and Risks
Trichomoniasis symptoms and risks differ notably between men and women, with women experiencing more frequent and severe manifestations. Men are often asymptomatic carriers, facilitating silent spread.
Symptoms Comparison
Aspect
Women
Men
Common Signs
Frothy, foul-smelling (fishy) vaginal discharge (yellow/green/white); genital itching, burning, redness, soreness, pain during sex or urination; lower abdominal pain
Itching/irritation inside penis; burning after urination/ejaculation; penile discharge (froth-like); rare urethral discomfort or frequent urination
Frequency
30% to 50% symptomatic; appears 5 to 28 days post-exposure.
<30% symptomatic; often mild or absent.
Risk Comparison
Women face higher complication risks like pelvic inflammatory diseases, infertility, ectopic pregnancy, preterm birth, and 1.5–3X increased HIV acquisition from mucosal inflammation. Men risk prostatitis, epididymitis, urethritis, or infertility (less common), plus elevated HIV transmission if co-infected. Both genders see heightened HIV susceptibility, but women’s genital changes amplify it more.
E) How is Trichomoniasis Diagnosed Differently in Men and Women
Trichomoniasis diagnosis differs between men and women mainly due to anatomical differences and parasite load, with women easier to test via vaginal samples. Men often require urine or urethral swabs since the infection is urethral and frequently asymptomatic.
Sample Collection
Women typically provide vaginal swabs (self-collected or clinician-obtained) or endocervical samples during pelvic exams, capturing higher parasite concentrations. Men use first-void urine, urethral swabs or semen as vaginal sampling doesn’t apply.
Testing Methods Comparison
Method
Women
Men
Notes
Wet Mount Microscopy
Vaginal fluid; sees motile parasites (50% to 70% sensitive)
Urine/urethral swab; lower yield due to fewer parasites
Quick but least accurate overall
NAAT/PCR
Vaginal swab/urine; >95% sensitive/specific
Urine/urethral swab; 98% detection in partners
Gold standard for both; preferred for low-load cases
Culture
Vaginal swab; 75% to 95% sensitive e.g. Diamond medium
Urethral swab/urine; slower, 20% to 70% yield
More reliable in women; multiple samples improve men’s results
NAAT is recommended for both genders in high-risk or asymptomatic screening, with follow-up testing more routine for women.
F) Role of Trichomoniasis in HIV Transmission from Women to Men
Trichomoniasis plays a significant role in facilitating HIV transmission from infected women to their male partners by increasing genital HIV shedding and mucosal inflammation. Effective treatment of the parasite can substantially mitigate this risk.
Mechanisms in Women to Men Transmission
In HIV positive women, Trichomoniasis vaginalis infection causes vaginal and cervical inflammation, elevating local HIV viral loads (e.g. by 0.5 to 1 log10 copies/ml in genital secretions) and promoting viral shedding into vaginal fluid. This exposes male partners to higher infectious doses during unprotected vaginal sex, as the parasite disrupts epithelial barriers and alters vaginal pH/flora, aiding HIV cell entry in penile/urethral mucosa.
Evidence and Impact
Studies estimate T. vaginalis contributes to 23% of HIV transmissions from women in high-prevalence settings, with co-infection linked to 747 annual new cases in U.S. women-to-partners scenarios. Treatment reduces shedding beyond antiretroviral therapy alone, potentially halving transmission risk; one model project 159 million yearly U.S. savings from routine screening/treatment in HIV+ women. African-American communities show amplified effects due to higher co-prevalence.
G) Role of Trichomoniasis in HIV Transmission from Men to Women
Trichomoniasis in men increases HIV transmission risk to women mainly through urethral inflammation and elevated seminal HIV viral loads. Treating male infections reduces this risk by resolving genital pathology.
Mechanisms in Men to Women Transmission
T. vaginalis causes urethritis and prostatitis in men, boosting HIV concentrations in urethral secretions and semen (up to 100 fold higher viral loads documented), which women encounter during vaginal sex. The parasite disrupts mucosal barriers and induced cytotoxic immune responses, enhancing HIV release from infected cells and degrading protective proteins like SLPI that block viral attachment.
Evidence and Impact
Studies link male trichomoniasis to higher female HIV acquisition rates, with co-infection amplifying transmission in high-prevalence areas; one review notes substantially increased urethral HIV shedding in affected men. While less studied than female to male direction, models suggest routine screening/treatment in men could curb heterosexual spread, especially in African-American or sub-Saharan communities.
H) Difference Between Treponema pallidum and Trichomoniasis
Treponema pallidum and Trichomonas vaginalis are both sexually transmitted infections (STIs), but they differ significantly in their causative agent type, symptoms, diagnosis, and treatment.
Treponema pallidum is a bacterium (spirochete) that causes syphilis while Trichomonas vaginalis is a protozoan parasite that causes trichomoniasis.
Key Differences
Feature
Treponema pallidum (syphilis)
Trichomoniasis (Trichomonas)
Pathogen Type
Bacterium (Spirochete)
Protozoan Parasite
Primary symptoms
Painless, firm chance ulcer
Vaginal/urethral itching, discharge, pain
Discharge
Rare
Yellow-green, frothy, fishy odour
Progression
Chronic, progresses in stages (primary → tertiary)
Acute, usually does not progress to chronic disease
Diagnosis
Blood tests (RPR/VDRL or Treponemal tests)
Microscopic inspection, wet mount, or PCR
Treatment
Penicillin (Often)
Metronidazole or Tinidazole
Long-term Risk
Damage to brain, nerves, heart (if untreated)
Increased risk of HIV; rarely chronic
Pathogen and Structure
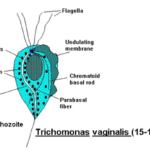
T. Pallidum is a thin, spiral-shaped bacterium (spirochete) that cannot be easily grown in culture, while Trichomonas vaginalis is a flagellated, motile protozoan parasite.
Symptoms
Syphilis often presents as a single, painless, hard ulcer (chancre) at the site of infection, while trichomoniasis is characterized by severe itching, burning, and a foul-smelling, yellow-green vaginal discharge in women, while men are often asymptomatic.
Stages
Syphilis is divided into stages primary, secondary, latent and tertiary and can last for years, causing systemic damage. Trichomoniasis does not have stages.
Transmission
Both are transmitted through sexual contact, but syphilis can also be passed vertically from mother to child (Congenital syphilis).
Treatment
They require completely different antibiotic/antiprotozoal medications; treatment for one will not cure the other.