Pancreatic cancer is a malignant tumor that forms in the tissues of the pancreas and is often aggressive and hard to detect early. It typically arises from cells in the pancreatic ducts or endocrine glands, leading to a poor prognosis if advanced.
Definition
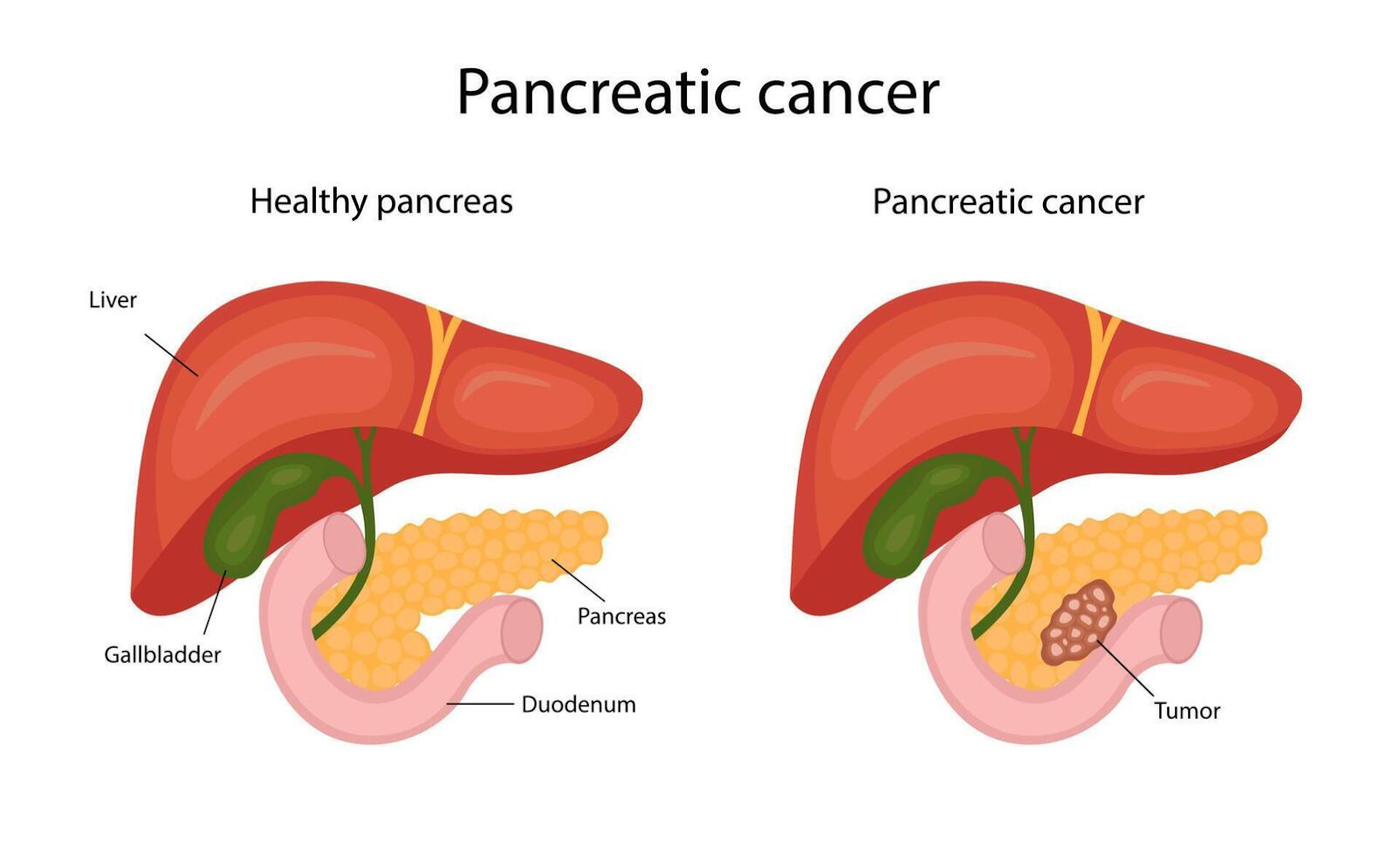
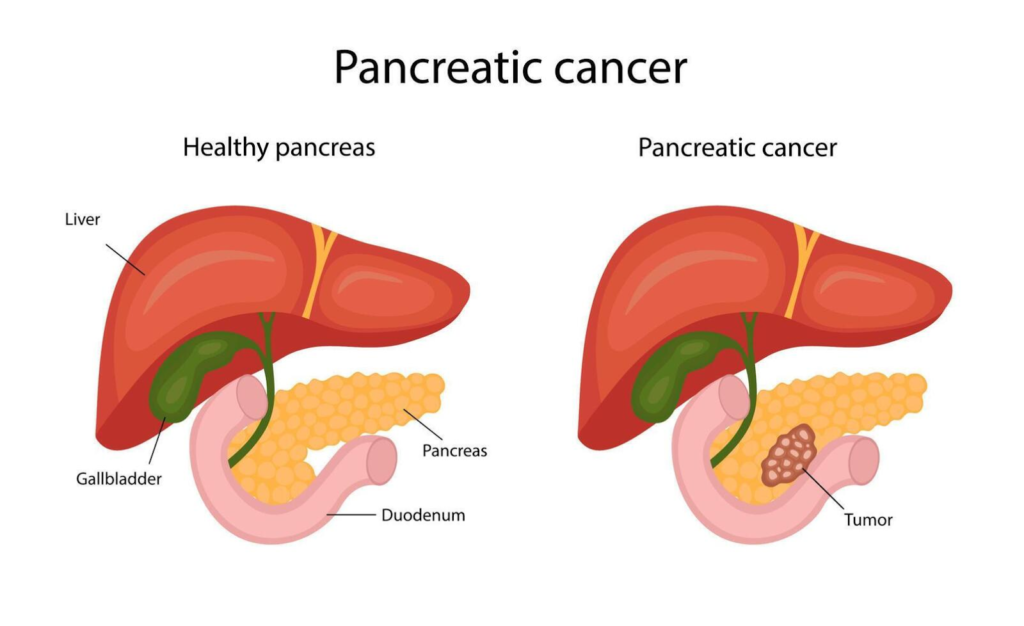
Pancreatic cancer refers to uncontrolled cell growth in the pancreas, a gland behind the stomach that aids digestion and blood sugar regulation. In most cases, about 90% to 95% are exocrine tumors starting in enzyme-producing cells, while rare types originate in hormone-producing endocrine cells.
Causes
Key risk factors include smoking, obesity, type 2 diabetes, chronic pancreatitis, heavy alcohol use, family history, and genetic mutations like BRCA2 or Lynch syndrome. Environmental exposures to chemicals such as asbestos or pesticides may also contribute.
Modifiable Risk Factors
These account for about 40% to 50% of cases and can be addressed through lifestyle changes.
- Smoking doubles the risk; quitting reduces it over time
- Obesity, especially abdominal fat, raises risk by 20%; high-fat, low-fiber diets with red/processed meats contribute
- Heavy alcohol use (> 3 drinks daily) is linked to chronic pancreatitis and higher odds
- Diabetes, especially new-onset type 2 and chronic pancreatitis, increases risk significantly
- Chronic pancreatitis from alcohol and smoking inflames the pancreas long-term.
- Cirrhosis, pylori infection, and cystic fibrosis elevate odds
- Occupational exposures to chemicals
- Genetic and family factors of pancreatic cancer or syndromes like BRCA, Lynch syndrome, FAMMM, PALB2, Peutz-Jeghers increase risk
Main Types
Exocrine tumors (93% of cases)
Primarily pancreatic ductal adenocarcinoma, aggressive and fast-growing, starting in duct-lining cells.
Neuroendocrine tumors (NETs) (3% to 5% of cases)
Slower-growing, functional types release hormones (e.g., insulinomas causing low blood sugar); non-functional types do not.
Symptoms
Early symptoms are rare; advanced signs include abdominal/back pain, unexplained weight loss, jaundice (yellow skin/eyes), dark urine, light stools, loss of appetite, new-onset diabetes, fatigue, and bloating.
Diagnosis
Diagnosis involves assessing tumor size, lymph node involvement, and spread via staging (0 to 4). Confirmation uses biopsy, blood tests (e.g., CA19-9), and imaging to determine resectability.
Diagnosis Methods
Imaging:
CT/MRI scans, endoscopic ultrasound (EUS), and ERCP.
Biopsy:
Fine needle aspiration during EUS.
Other:
PET scans and SpyGlass cholangioscopy for detailed views.
Prevention Measures
Quit smoking (reduce risk significantly), maintain a healthy weight via a plant-based diet and exercise, limit alcohol, and screen high-risk individuals, e.g., those with genetic mutations.
Control Measures
Early detection through screening high-risk groups, timely treatment to downstage disease, and managing comorbidities like diabetes. In India, NPCDCS promotes screenings for common cancers, adaptable to pancreatic via risk awareness.
Treatment
Options depend on stage: surgery (Whipple procedure, pancreatectomy for resectable cases), chemotherapy (FOLFIRINOX, gemcitabine-nab-paclitaxel), radiation, targeted therapies (e.g., PARP inhibitors for BRCA mutations), and clinical trials.
Public Awareness
Campaigns use posters, digital ads, GP education, and patient stories to highlight symptoms and risks, as low awareness delays diagnosis. Efforts like Pancreatic Cancer Aware distribute resources to boost early help-seeking.
Community Engagement
Involves patient-researcher partnerships, events, and sharing findings for bidirectional learning to address barriers and empower communities.
IEC Materials
Information, education, and communication tools include symptom posters, fact sheets, e-learning for GPs, and serious games/apps for symptom recognition and knowledge retention.
Role Of Public Health Department
Public health departments fund research, run screening programs (e.g., NPCDCS in India for NCDs/cancers), promote tobacco control/vaccinations, ensure access to care/trials, and lead awareness via policy and community education.
Prognosis and Survival Rates for Pancreatic Cancer
Pancreatic cancer has one of the lowest survival rates among cancers due to its late diagnosis and aggressive nature. The overall 5-year relative survival rate is around 13% as of 2026, with significant variation by stage. The combined 5-year survival for all stages and types is 13%, up from 7% a decade ago, reflecting modest treatment advances. For the most common form, pancreatic ductal adenocarcinoma, it’s about 8%. These rates are based on large U.S. databases like SEER, covering diagnoses from 2015 to 2021.
Prognosis Factors
Surgery-eligible cases (15% to 20% of diagnosis)
5-year survival can exceed 20% to 80% post resection, like with the Whipple procedure, with median survival of 15 to 20 months.
Positive influences:
Early detection, good performance status, CA19-9 response to chemo, no major comorbidities.
Negative:
Age over 70, diabetes, high tumor grade, mutations like KRAS.
Median survival without treatment is 3-4 months; with chemo, 6-12 months for advanced disease.
Progress continues via trials, but early detection remains key to improving outcomes.
Palliative Care for Pancreatic Cancer
Pancreatic cancer palliative care focuses on improving quality of life for advanced-stage patients by managing symptoms like pain, jaundice, obstruction, and nutritional issues, rather than curing the disease.
Goal
Early integration of palliative care alongside active treatment enhances comfort, reduces hospital stays, and may extend survival while addressing emotional and psychological distress. It involves multidisciplinary teams including oncologists, nurses, pain specialists, nutritionists, and social workers.
Symptom Management
Pain relief:
Celiac plexus nerve blocks, opioids, and radiation to shrink tumors pressing on nerves.
Obstructive Jaundice:
Biliary stents or surgery to bypass blockages, restoring bile flow and easing itching and fatigue.
Gastric outlet obstruction:
Stents or gastrojejunostomy to maintain nutrition and prevent vomiting.
Other:
Anti-nausea meds, appetite stimulants, paracentesis for ascites, and VTE prophylaxis.
Psychological Support
Includes advanced care planning, hospice referral, family counseling, and spiritual care to align treatments with patient goals, reducing end-of-life aggression like ICU admissions.
Home-Based Palliative Care
Home-based palliative care for pancreatic cancer patients emphasizes comfort, symptom control, and support in familiar surroundings, often via hospice programs when life expectancy is under 6 months. It integrates medical, emotional, and practical services delivered by multidisciplinary teams through regular home visits.
Hospice Services at Home
Hospice, the primary model for home-based end-of-life care, provides:
- Nursing visits for pain management, wound care, and symptoms relief
- Medical supplies/equipment, e.g., bedpans, hospital beds, wheelchairs, oxygen
- Medications and therapy (e.g., physical, occupational, speech, and crisis care)
- Home health aides for bathing, grooming, light housekeeping and meal prep
- Volunteers for errands, childcare, respite, and companionship
Most care is delivered at home with family caregivers supported by hospice teams like doctors, nurses, aides, social workers, chaplains, and volunteers.
Staging Of Pancreatic Cancer
Pancreatic cancer staging uses the AJCC TNM system to assess tumor extent, lymph node involvement, and metastasis, guiding treatment and prognosis. It primarily applies to the common exocrine type, with stages 0 to IV based on imaging, biopsy, and surgery findings.
TNM Components
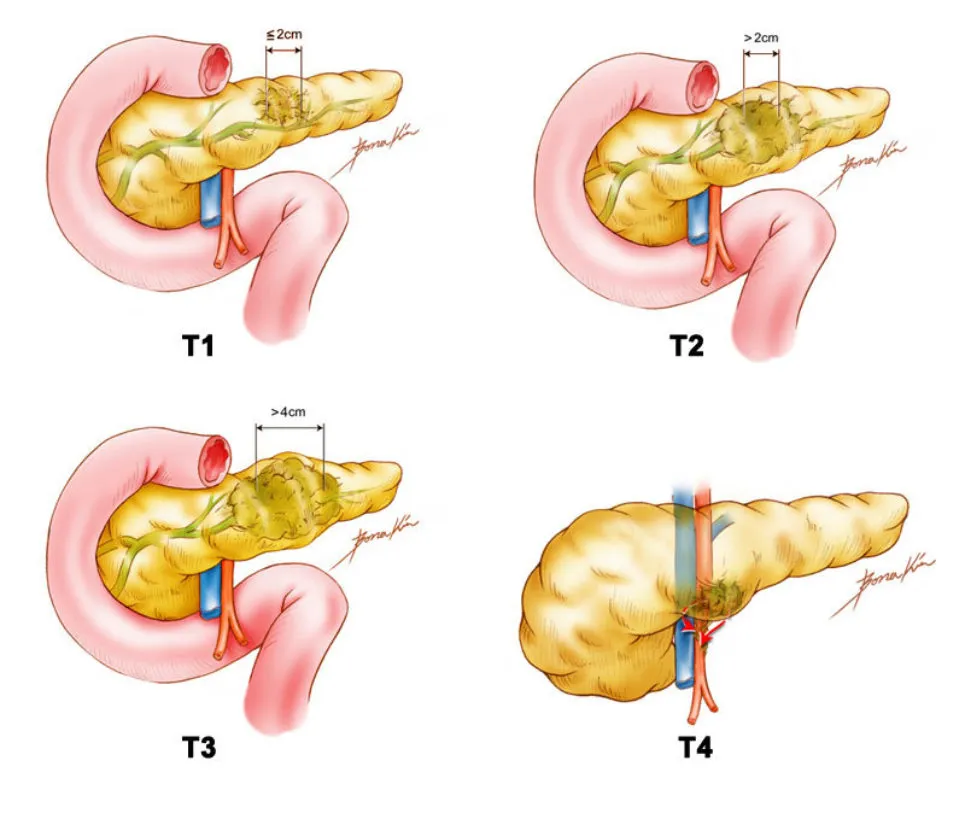
T (Tumor): Size and local invasion
- TX: Cannot be assessed
- TO: no primary tumor
- TiS: Carcinoma in situ (stage 0)
- T1: < 2 cm
- T2: >2 cm – 4 cm, pancreas-confined
- T3: >4 cm or extend beyond pancreas
- T4: Involves major arteries
N (Nodes): Lymph node spread
- NO: None
- N1: 1-3 regional nodes
- N2: >4 regional nodes
M (Metastasis): Distant spread
- MO: None
- M1: Distant sites, e.g., liver, peritoneum, lungs