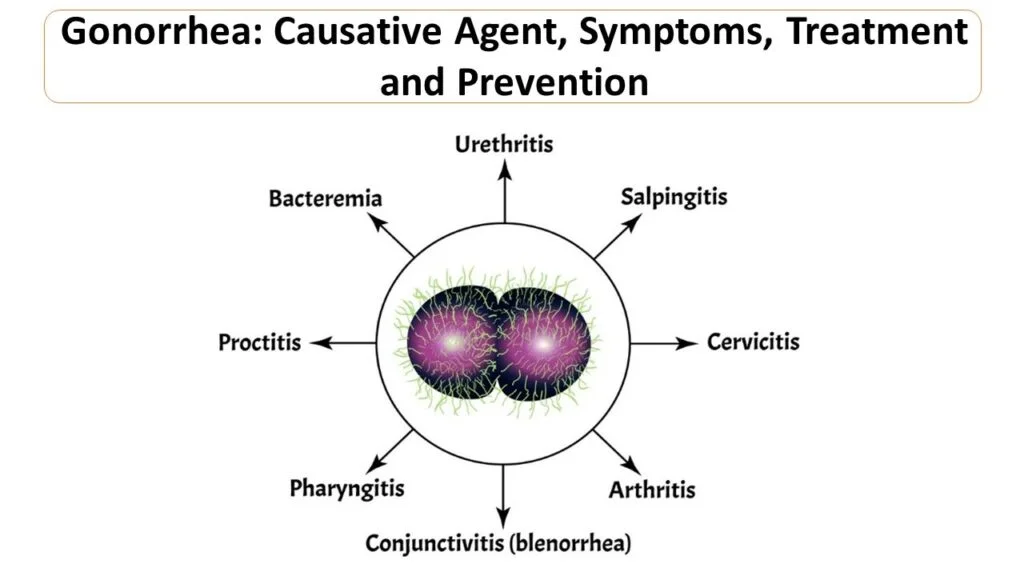
Gonorrhea is a common, preventable, and curable sexually transmitted infection (STI) caused by the bacterium Neisseria gonorrhoeae. It primarily spreads through unprotected vaginal, anal, or oral sex and can lead to serious complications if untreated.
Definition
Gonorrhea, also known as the clap, infects the genitals, rectum, throat, or eyes via sexual contact or from mother to child during birth. It does not confer immunity, allowing reinfection.
Causes
The sole cause is infection with Neisseria gonorrhoeae, transmitted mainly through sexual contact with an infected person. Vertical transmission to newborns can cause eye infections.
Main Types
Gonorrhea is classified by location:
- Urogenital (genital tract in men / women)
- Extragenital (rectal, pharyngeal, conjunctival)
- Disseminated (systemic, affecting joints / skin)
Symptoms
Many cases are asymptomatic, especially in women; men often have penile discharge, burning urination, or testicular pain. Women may experience vaginal discharge, bleeding or pelvic pain; anal / throat infections cause discharge, soreness or sore throat.
Diagnosis
Diagnosis relies on molecular tests (NAATs) from urine or swabs as the gold standard. Gram stain microscopy aids symptomatic cases; syndromic management is used where labs are unavailable.
Diagnostic Methods
NAATs target bacterial genes (e.g. APTIMA, BD probe Tec.), culture for resistance testing; screening for high-risk groups.
Prevention Measures
Use condoms consistently, limit partners, test regularly, and notify partners. Newborn eye ointment prevents neonatal infection.
Control Measures
Screen high-risk groups, partner notification, syndromic treatment per guidelines, and resistance surveillance like EGASP.
Treatment
The preferred treatment is a single intramuscular Ceftriaxone injection (500mg for most adults), which achieves high cure rates over 99% for urogenital, rectal and pharyngeal infections. Or cefixime plus azithromycin; test-of-cure needed due to resistance risks. Resistance monitoring is critical, with new oral options like gepotidacin and zoliflodacin recently approved. Abstain from sex for 7 days post-treatment or until symptoms resolve and partners are treated. Gonorrhea is effectively treated with antibiotics, primarily cephalosporins, due to rising resistance in the bacterium Neisseria gonorrhoeae. Prompt treatment cures uncomplicated cases in most patients, but follow-up-testing is often required.
When ceftriaxone is unavailable or not tolerated, oral cefixime (800 mg single doses) plus azithromycin is used, though less effective for pharyngeal gonorrhea. For cephalosporin allergies, gentamicin 240 mg IM plus azithromycin 2 g oral serves as an alternative.
Partner Treatment
Partner Treatment for gonorrhea contacts known as Expedited Partner Therapy (EPT) or Patient-Delivered Partner Therapy (PDPT), involves providing antibiotics to sexual partners without their prior clinical evaluation to prevent reinfection and curb spread. CDC recommends evaluating and treating partners with sexual contact within 60 days of the patient’s symptoms or diagnosis. Preferred EPT regimen for partners; cefixime 800 mg orally as single dose, if chlamydia co-infection is excluded in the patient.
Magnitude and Global Burden
In 2020, WHO estimated 82.4 million new cases globally among adults 15 to 49, with 0.9% prevalence in women and 0.7% in men. Antimicrobial resistance threatens untreatability.
Burden in India
Gonorrhea imposes a notable disease burden in India, particularly among high-risk groups, though national incidence data remains limited due to reliance on syndromic reporting. Prevalence of curable STIs, including gonorrhea, is under 4% in the general population, with gonorrhea often below 1% in the community surveys. Prevalence varies; high in key populations like MSM (up to 14.8% in some studies), lower in community samples (0.07%) interventions reduced cases significantly in areas like Karnataka. NACO interventions have reduced cases in targeted areas, but under-reporting and asymptomatic infections inflate true burden.
Gonorrhea Prevalence Data
Gonorrhea prevalence varies significantly across Indian states, with limited comprehensive up to date national data due to reliance on syndromic surveillance and targeted studies in high-risk groups rather than uniform population screening. Studies show higher rates in urban and high-risk populations.
Andhra Pradesh
Gonorrhea prevalence around 0.05% in general population, up to higher in high-risk groups; pooled with Odisha at low levels.
Maharashtra
(e.g. Mumbai) Up to 9.3% among brothel-based FSWs in earlier surveys (2005 to 2007), though declining trends noted.
Telangana
6.4% gonorrhea in FSWs from IBBA-1 study.
Odisha
Pooled low prevalence in general population meta analysis.
Public Health Role
India’s NACO provides free STI clinics, colour-coded drugskits, syndromic / presumptive treatment, and peer outreach via Avahan. Public health departments promote condoms, screening, and resistance monitoring.
Awareness and Engagement
Condom promotion campaigns raised awareness to 98% in some studies; peer education targets sex workers / MSM. Community interventions empower high-risk groups.
ICE Materials
NACO supplies drug kits and uses posters / leaflets for STI education in clinics and targeted interventions.
Complications of Untreated Gonorrhea
Untreated gonorrhea can lead to severe, long-term serious health issues in both men and women due to its often asymptomatic nature, including infertility and increased HIV risk.
In Women
Gonorrhea often ascends to cause pelvic inflammatory disease (PID), scarring fallopian tubes and leading to infertility, ectopic pregnancy, or chronic pelvic pain. It may also result in abscesses, Fitz-Hugh-Curtis syndrome (liver inflammation) or life-threatening complications during pregnancy like miscarriage.
In Men
Epididymitis causes testicular swelling, pain, and potential infertility; prostatitis or urethral strictures can also develop. Systemic spread raises prostate cancer risk.
Systemic Effects
Disseminated gonococcal infection (DGI) affects 0.6% to 3% of women and 0.4% to 0.7% of men, causing septic arthritis, skin lesions, meningitis, or endocarditis. Neonatal eye infections from mother to child transmission can lead to blindness. Untreated cases heighten HIV susceptibility and rarely, reactive arthritis. Prompt treatment prevents most complications.
High-Risk Groups
Gonorrhea rates in high-risk groups like female sex workers (FSWs), men who have sex with men (MSM) and transgender individuals (TG) vary by state in India, based mainly on NACO’s integrated Behavioural and Biological Assessment (IBBA) rounds and recent studies. Data is district-specific rather than state-wise with decline noted over time due to interventions.
Statewise Data
| State | Group | Gonorrhea Prevalence (%) | Year / Source |
|---|---|---|---|
| Telangana | FSWs | 6.4 % | IBBA-1 (2005-2007) |
| Maharashtra (Mumbai, brothel-based) | FSWs | 9.3 % | IBBA-1 |
| Maharashtra (Mumbai) | MSM | 14.8 % (facility based) | Recent study |
| Tamilnadu (Chennai) | MSM | 0.07 % (community) | Cross-sectional |
| Tamilnadu (Chennai) | MSM | 37.8% any STI (incl. gonor. than Chennai’s) | 2020 study |
| Andhra Pradesh | FSWs | 0 to 19 % range in studies | Meta-analysis |