
Introduction to Chandipura Encephalitis Virus
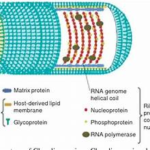
The Chandipura encephalitis virus, often associated with Chandipura encephalitis, has its origins traced to 1965, when it was first isolated from the blood of two febrile adults in Chandipura village, Nagpur district, Maharashtra, India. It belongs to the Rhabdoviridae family, genus Vesiculovirus, and is closely related to vesicular stomatitis virus.
The CHP virus was discovered by NIV from a serum sample of a patient collected during an outbreak of febrile illness in the Nagpur area of Maharashtra state, India, in 1965. The virus was not assigned any public health importance until 2003, when an investigation conducted by NIV associated the CHP virus with a large encephalitis outbreak in children in many districts of Andhra Pradesh & Maharashtra, India.
Early Discoveries and Epidemiological Expansion
After its discovery, Chandipura virus cases were found in Central India in 1980, including Madhya Pradesh. Sandflies (genus Phlebotomus) are the primary vectors, as confirmed by later outbreaks where the virus was detected in sandflies collected near affected patients.
The virus gained global attention following major outbreaks in children during 2003 in Maharashtra & Andhra Pradesh, which resulted in over 300 deaths, having a high fatality rate often exceeding 50%.
Geographic Distribution and Global Presence
Although human cases have been documented almost exclusively in India, especially in central & southern states like Maharashtra, Madhya Pradesh, Andhra Pradesh, Gujarat, Bihar, Karnataka, Tamil Nadu, Odisha, & Kerala, there is evidence that CHPV has a wider geographic presence.
The virus or viral RNA has been isolated from sandflies in parts of Africa (Senegal, Nigeria, and Kenya), indicating that CHPV or closely related viruses exist outside India. Antibodies to CHPV have also been found in macaques in Sri Lanka, suggesting a possible broader range in Asia.
Human infections and encephalitis outbreaks have not been reported beyond India & Sri Lanka, but the presence of the virus in wild arthropods & mammals in Africa suggests an extended geographical distribution by sandfly vectors such as Phlebotomus & Sergentomyia species and possibly other arthropods like mosquitoes & ticks. No evidence currently exists of human-to-human transmission.
Magnitude of Problem of CHPV
Public Health Impact of Chandipura Virus
The magnitude of Chandipura virus (CHPV) infection and outbreaks in India has been significant, with several major epidemics and a high case-fatality ratio. (CFR). Key details on the magnitude of CHPV include
Key Outbreaks and Case Fatality Rates
- The largest outbreak recorded was in 2003-2004, affecting 1 district in Andhra Pradesh and 11 districts in Maharashtra & Gujarat; around 329 cases were reported with approximately 183 deaths. This outbreak notably affected children and caused severe encephalitis with rapid progression to death. The CFR in these outbreaks is about 56%.
- Since then, several smaller outbreaks and sporadic cases have been reported in western, central, & southern India. The CFR in these outbreaks has ranged from 28% to as high as 79%, mostly affecting children under 15 years.
- In 2024, the largest outbreak in 20 years occurred, particularly in Gujarat, with 245 cases of acute encephalitis syndrome, including 82 deaths, yielding a 33% CFR.
- Other outbreaks in various states like Maharashtra, Gujarat, Rajasthan, and Bihar have reported hundreds of cases cumulatively over the years with consistent high mortality.
Clinical Severity and Challenges
- CHPV causes severe acute encephalitis in children, with symptoms like fever, vomiting, convulsions, & coma, and death often occurs within 24-48 hours after symptom onset.
- There is no specific antiviral treatment or vaccine for CHPV, making clinical management primarily supportive, contributing to the high mortality.
- CHPV remains endemic in India, with periodic outbreaks coinciding with monsoon and post-monsoon seasons favorable to sandfly vectors.
Conclusion and Global Burden
The CHPV poses an ongoing challenge due to the absence of targeted therapeutics or preventative vaccines. This overview highlights the critical need for enhanced surveillance, vector control, personal protection, awareness, and research into vaccines and treatments to mitigate CHPV’s burden.
The global burden of CHPV encephalitis is not precisely quantified due to limited surveillance and geographical concentration, but available data indicate a significant public health impact primarily in India and parts of South Asia. Outside India, detection has occurred sporadically in Sri Lanka, Nepal, and African countries.