Human papillomavirus (HPV) is a group of more than 100 related DNA viruses that infect the skin and mucous membranes, primarily causing warts and some types of cancers. It is the most common sexually transmitted infection worldwide. HPV is classified into low-risk (non-cancerous) and high-risk (oncogenic) types based on their potential to cause cancer. It includes over 200 strains, most of which are harmless and clear on their own.
Virus Basics—Human Papillomavirus
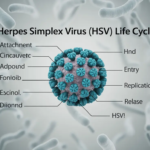
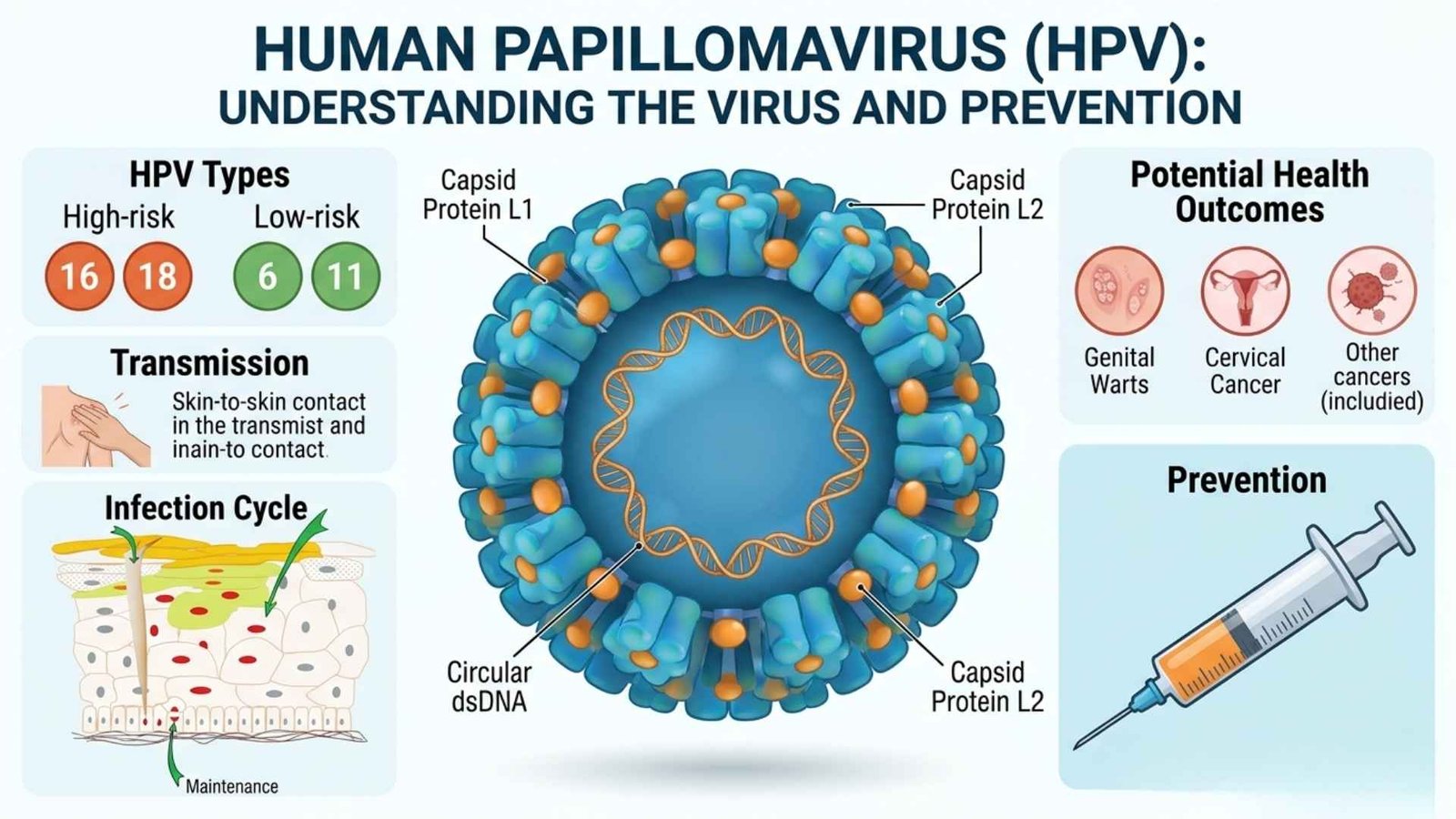
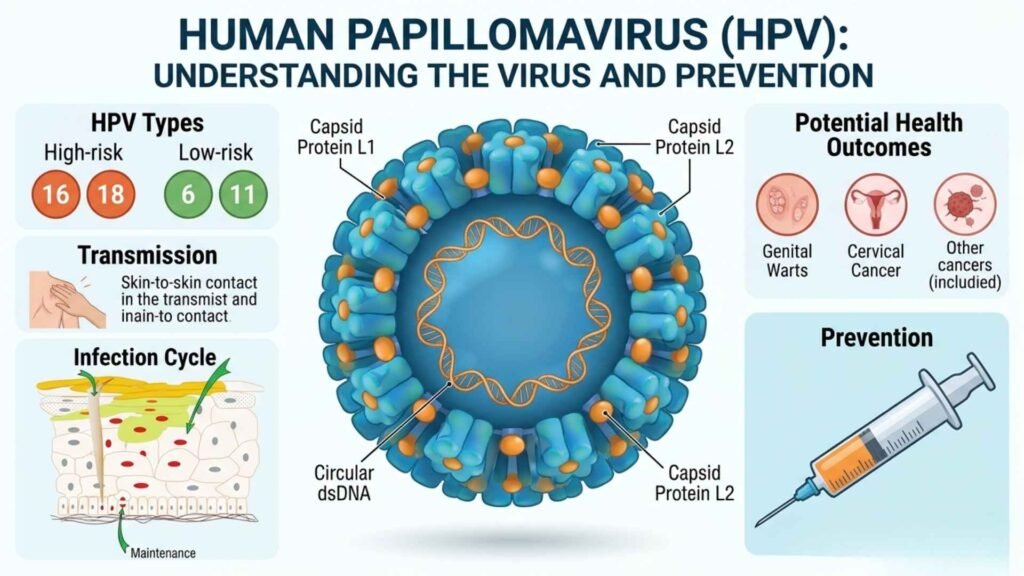
HPV is a small, non-enveloped DNA virus from the Papillomaviridae family with a circular 8-kb genome. It encodes early proteins for replication and late proteins (L1, L2) for structure. The virus infects basal cells of epithelium after skin or mucosal disruption.
Causes and Transmission
HPV is transmitted through direct skin-to-skin contact, most commonly during vaginal, anal, or oral sex.
It can also spread through intimate contact without penetrative sex and from mother to baby during childbirth in rare cases.
The virus enters the basal epithelial cells through micro-abrasions in the skin or mucosa.
Main Types of HPV
HPV is divided into:
| Category | Main Types | Typical organs affected | Notes |
|---|---|---|---|
| Low-Risk | HPV 6, 11, 40, 42, 43, 44 | Genitals (vulva, penis, cervix, and vagina), anus, mouth & throat | Cause genital warts & benign lesions |
| High-risk | HPV-16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68 | Cervix, vulva, vagina, penis, anus, Oropharynx (tongue, tonsils) | Cervical dysplasia and cancers; 13-14 types are classified as high-risk oncogenic types. |
| Other high-risk | HPV—31, 33, 45, 52, 58, etc. (and sometimes 35, 39, 51, 56, 59, 66, 68, as additional high-risk | Cervix, vulva, vagina, penis, Anus , Oropharynx | Account for a smaller share of HPV-related cancers, about 15% of cervical cancers. |
Symptoms
Asymptomatic carrier: Many people show no symptoms; HPV clears on its own.
Genital Warts: Small, flesh-colored, cauliflower-like growths on genitals, anus, or nearby areas (caused by HPV 6/11).
Recurrent respiratory papillomatosis: Warts in the larynx causing hoarseness or breathing difficulty (rare).
Cancer-related signs (late): abnormal vaginal bleeding, pelvic pain, or foul discharge (cervical cancer). Persistent sore throat, hoarseness, neck lump, and difficulty swallowing (oropharyngeal cancer).
Diagnosis and Diagnostic Methods
Clinical examination: Visual inspection for genital warts or cervical lesions.
Pap Smear (Pap test): Cervical cell sampling to detect precancerous or abnormal changes.
HPV DNA testing: A molecular test (PCR or hybridization) on cervical swabs to identify high-risk HPV types, e.g., 16 and 18.
Colposcopy and biopsy: Magnified examination of the cervix and tissue biopsy if the Pap or HPV test is abnormal.
Anogenital / oropharyngeal swabs: For genital warts or oral HPV detection in selected cases.
Treatment
No cure for the virus itself, but symptoms and lesions can be treated.
Genital warts: Topical agents (podophyllotoxin, imiquimod, trichloroacetic acid). Physical removal (cryotherapy, electrocautery, laser, and excision).
Precancerous lesions (cervix): LEEP (loop electrosurgical excision), excision, cryotherapy, or cone biopsy.
Cancers: Surgery, radiotherapy, chemotherapy, or targeted therapy depending on site and stage.
Prevention and Control Measures
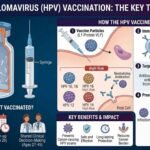
HPV vaccination: Vaccines (e.g., bivalent, quadrivalent, 9-valent) protect against HPV 16/18 and, in some cases, 6/11 and other high-risk types. Recommended for boys and girls ideally before sexual debut (9 to 14 years).
Safe sex practices: Consistent condom use reduces but does not eliminate transmission risk.
Screening programs: Regular cervical screening (Pap/HPV testing) detects pre-cancer early.
Public health control: High-coverage vaccination programs, organized screening, and linkage of positive cases to treatment.
Public Awareness and Community Engagement
Public awareness campaigns: Educate about HPV transmission, cancer risk, and benefits of vaccination and screening.
Community engagement strategies: Collaborate with schools, colleges, religious and community groups, and media for outreach. Use community health workers, ASHAs, and local leaders to counter myths and vaccine hesitancy.
IEC Materials
Print materials: posters, pamphlets, and booklets in local languages explaining HPV, cervical cancer, and vaccination.
Audio-visual: Radio spots, TV campaigns, and short videos demonstrating correct condom use and the importance of screening.
Digital content: Social media posts, WhatsApp messages, and websites with infographics in multiple languages.
Role of Public Health Department
Policy and program implementation: Introduce and scale up HPV vaccination in school- or community-based programs. Establish organized cervical cancer screening (Pap/HPV testing) and treatment services.
Surveillance and monitoring: Track HPV-related cancers, vaccination coverage, and screening outcomes.
Training and capacity building: Train doctors, nurses, and ASHAs on HPV, vaccination, screening, and counseling.
Coordination: Partners with NGOs, schools, media, and private providers to expand reach.
Magnitude and Global Risk of HPV
Over 100 HPV types circulate globally; about 40 infect anogenital regions.
HPV causes more than 25% of infection-related cancers worldwide, including the majority of cervical cancers.
Cervical cancer is the 4th most common cancer in women globally; almost all cases are HPV-driven.
Risk In India
India bears a high burden of HPV-related cancer, especially cervical cancer, which is the leading cancer in Indian women.
About 6.6% of women in the general population harbor cervical HPV infections; HPV 16 and 18 account for ~76% of cervical cancers.
Head and neck (especially oropharyngeal) cancers show regionally variable HPV prevalence, with higher rates in eastern India.
Risk in Maharashtra (including Nagpur)
Maharashtra has a moderate-to-high HPV-related cancer burden, especially in urban and peri-urban areas due to population density and lifestyle factors.
Cervical cancer incidence in Maharashtra is significant, though below the highest rates in eastern states; it remains a major public health concern.
Oropharyngeal cancer studies in India show lower HPV prevalence in the western region (around 12%) compared with the east (about 58%), indicating relatively lower HPV-driven HNC in Maharashtra.
Public health programs in Maharashtra (including Nagpur) are gradually rolling out HPV vaccination pilots and expanding cervical screening camps through urban health and district health initiatives.