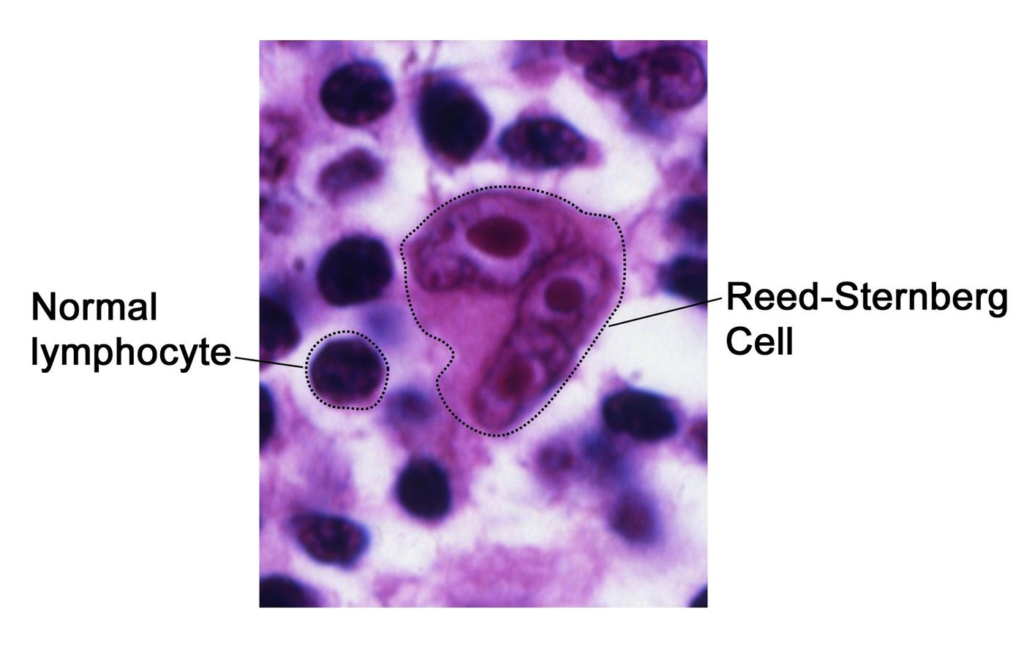
Non-Hodgkin lymphoma is a type of cancer that affects lymphocytes, which are white blood cells in the immune system. It differs from Hodgkin lymphoma by lacking Reed-Sternberg cells and often spreads unpredictably across lymph nodes and organs.
Non-Hodgkin lymphoma (NHL) is a group of blood cancers originating from abnormal lymphocytes, B-cells, T-cells, or NK-cells in the lymphatic system, excluding Hodgkin lymphoma. It can occur at any age but is more common in older adults, with B-cell types being far more prevalent than T-cell.
Definition
NHL involves uncontrolled growth of lymphocytes forming tumors in lymph nodes, the spleen, or other organs; over 70 subtypes exist, classified as indolent (slow-growing) or aggressive (fast-growing).
Causes
Exact cause unknown; risk factors include weakened immunity (HIV, organ transplants), infections (Epstein-Barr virus, hepatitis C, H. pylori), autoimmune diseases, obesity, age over 60, and certain chemicals or radiation.
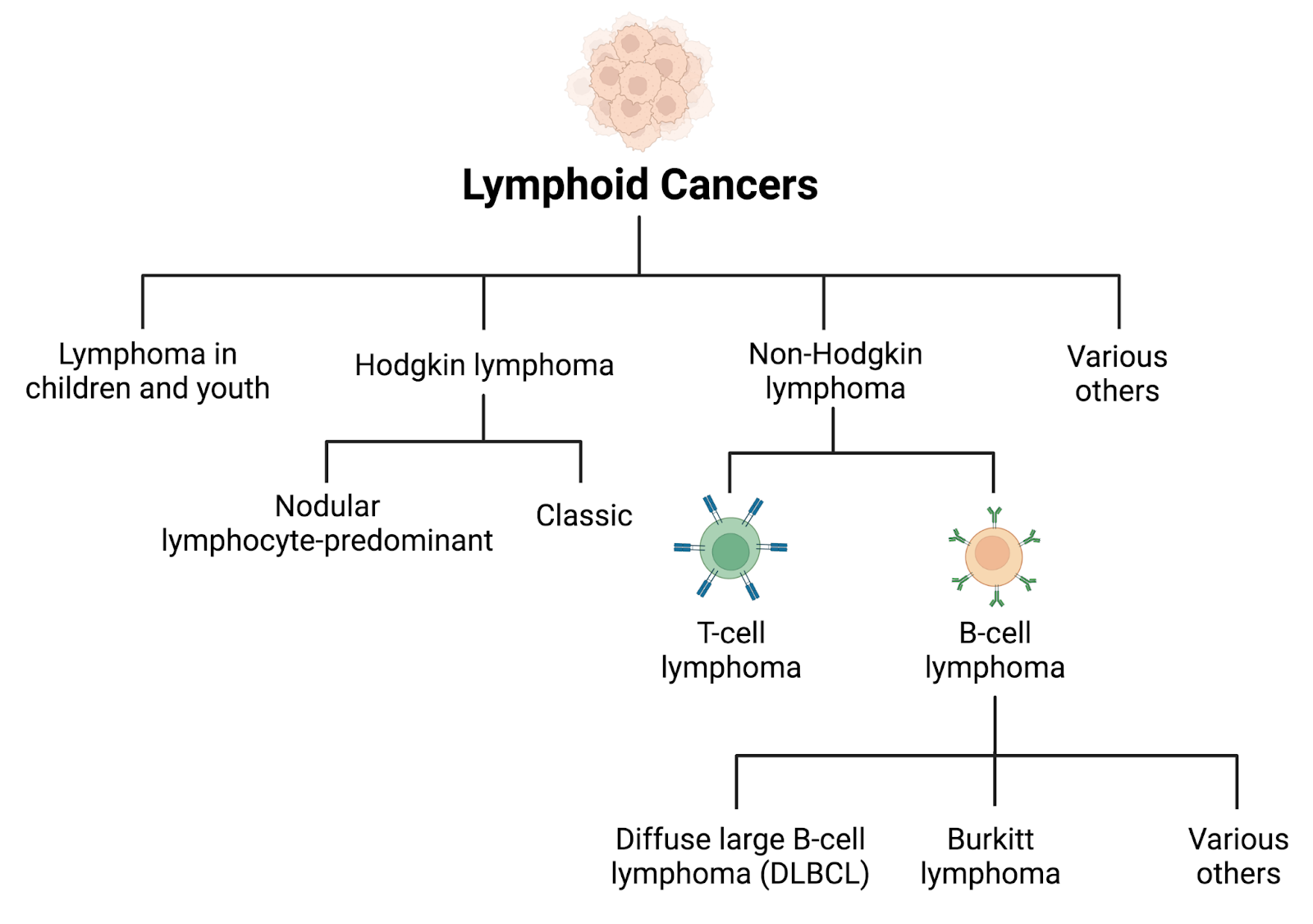
Main Types
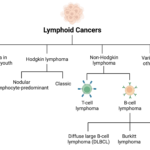
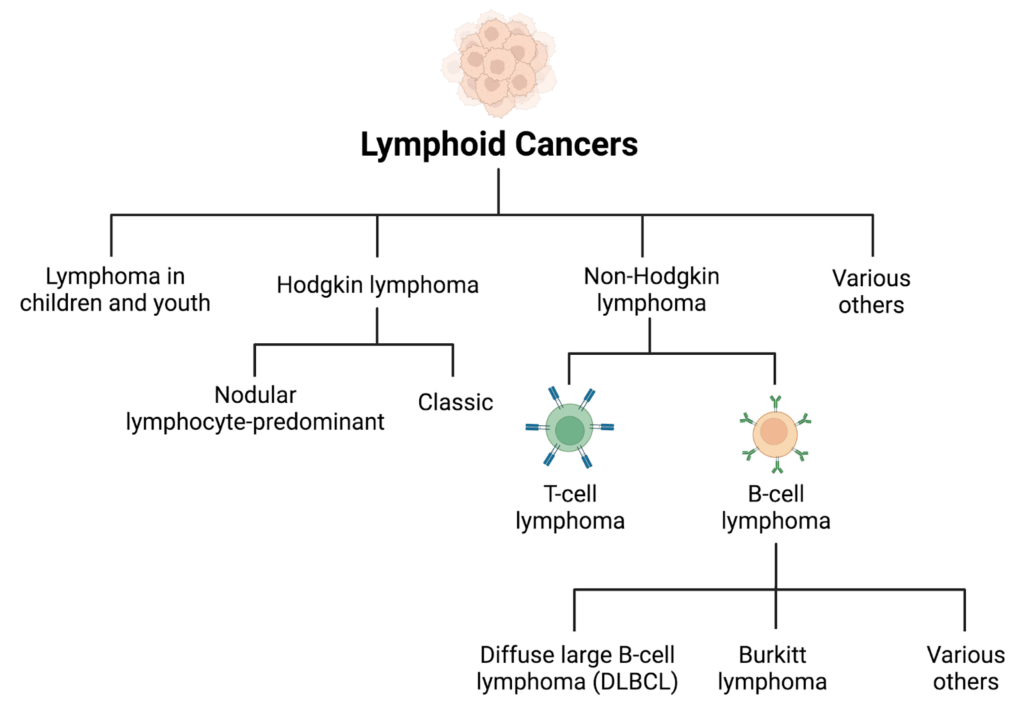
1) B-cell:
Diffuse large B-cell lymphoma (most common), follicular lymphoma, mantle cell, and marginal zone.
2) T-Cell:
Peripheral T-cell lymphoma and anaplastic large cell lymphoma are grouped by the WHO into indolent vs. aggressive.
Symptoms
Painless swollen lymph nodes (neck, armpits, groin), fever, night sweats, weight loss, fatigue, itching, bone pain, chest pain, or abdominal swelling. These arise as abnormal lymphocytes multiply and impair immune function.
Diagnosis
Physical exam for lymph node swelling, confirmed by biopsy (lymph node or bone marrow ) with immunohistochemistry to identify subtype and absence of Reed-Sternberg cells. Prognosis varies by subtype, stage, and patient factors.
Diagnostic Methods
Blood tests (CBC, LDH), imaging (CT/PET scans), bone marrow biopsy, lumbar puncture for CNS involvement, and molecular tests for genetic markers.
Prevention Measures
No guaranteed prevention; reduce risks by managing infections (HIV/hepatitis treatment), avoiding smoking/obesity, limiting chemical exposure, and promptly treating autoimmune conditions.
Control Measures
Early detection via screening for high-risk groups, infection control, healthy lifestyle (diet and exercise), and vaccination against preventable viruses like hepatitis B.
Treatment
Chemotherapy (e.g., R-CHOP), radiation, targeted therapy (rituximab), immunotherapy, CAR-T cell therapy, stem cell transplant, and watchful waiting for indolent types.
Public Awareness
September is NHL Awareness Month globally; campaigns emphasize symptoms, risk factors, and early detection through social media, health fairs, and survivor stories.
Community Engagement
Support groups and fundraising events (walks/runs). patient advocacy via organizations like the Lymphoma Research Foundation; volunteer-led education in communities.
IEC Material
Posters, brochures, and videos on symptoms/risks; digital toolkits from cancer societies, e.g., WHO/NCI, for schools/clinics. India-specific NCD materials include multilingual pamphlets on cancer prevention.
Role of Public Health Department
In India, the Ministry of Health and Family Welfare integrates NHL into NCD programs: surveillance, screening via Ayushman Bharat, awareness campaigns, training ASHA workers, subsidizing treatment, and health literacy initiatives.
Difference Between Blood Cancer and Non-Hodgkin Lymphoma cancer
“Blood cancer” is a broad term for cancers originating in the blood, bone marrow, or lymphatic system, including leukemia, lymphoma, and myeloma. Non-Hodgkin lymphoma (NHL) is a specific subtype of lymphoma, which itself is one category of blood cancer.
| Aspect | Blood Cancer (General) | Non-Hodgkin Lymphoma |
| Scope | Umbrella term for leukemia (blood-forming cells), lymphoma (lymphatic system), and myeloma (plasma cells). | Specific lymphoma type affecting lymphocytes without Reed-Sternberg cells. |
| Origin | Varies bone marrow (leukemia lymph nodes/organs (lymphoma) | Primarily lymph nodes, spleen, or other lymphatic tissues. |
| Cell Type | Abnormal blood cells, lymphocytes, or plasma cells. | Mostly B-cells or T-cells (over 70 subtypes) |
Overlap and Distinction
All lymphomas, like NHL, are blood cancers since they involve uncontrolled lymphocyte growth in the immune system. However, not all blood cancers are NHL—leukemia circulates abnormal cells in the blood, while NHL forms solid tumors in lymph tissues. NHL is far more common than Hodgkin lymphoma and often diagnosed later.
Prognosis and Survival Rates for NHL Cancer
Non-Hodgkin Lymphoma (NHL) survival rates vary widely by subtype, stage, age, and treatment response, with overall 5-year relative survival around 75% to 85% based on recent data. Prognosis improves with early-stage diagnosis versus advanced, younger age, and indolent subtypes; aggressive types respond better initially but relapse more.
Palliative Care for Non-Hodgkin Lymphoma Cancer
Palliative care for Non-Hodgkin Lymphoma (NHL) focuses on improving quality of life by managing symptoms, side effects, and emotional needs, often alongside active treatments like chemotherapy. It’s appropriate from diagnosis, especially for advanced or relapsed aggressive NHL, and intensifies at end-of-life when a cure isn’t possible. Early integration reduces hospitalizations and boosts hospice use.
Symptoms Management
Pain, fatigue, dyspnea: short-course radiation, low-dose chemo, opioids, or targeted drugs.
Nausea, itching, night sweats: medications and non-drug therapies like positioning or cooling.
Emotional distress: – Counseling, REMAP framework for goals-of-care talks.
Care Team and Services
Multidisciplinary: oncologists, palliative specialists, nurses, social workers, and chaplains. Includes home hospice for holistic support (physical, psychological, and spiritual). For older adults with aggressive NHL, focus on avoiding ICU stays; hypoalbuminemia predicts lower hospice use. Caregiver support and nonpharmacologic aids, e.g., glasses and sleep optimization, enhance comfort.
Staging of Non-Hodgkin Lymphoma Cancer
Non-Hodgkin Lymphoma (NHL) staging determines how far the cancer has spread, guiding treatment decisions. The primary system used is the Lugano classification, a modern update to the Ann Arbor system, dividing NHL into stages I through IV based on lymph node involvement and extranodal spread.
The Lugano system categorizes NHL as follows:
Stage I: Cancer in one lymph node region or a single extranodal site without nodal involvement.
Stage II: Two or more lymph node regions on the same side of the diaphragm, possibly with limited contiguous extranodal extension.
Stage III: Lymph nodes on both sides of the diaphragm, potentially including the spleen.
Stage IV: Widespread involvement of one or more distant organs outside the lymph system, such as bone marrow, liver, or lungs.
Grading
NHL is also graded by cancer cell appearance and growth rate:
Low grade (indolent):- Slow-growing, like follicular lymphoma; may not require immediate treatment.
Intermediate/high-grade (aggressive):- Fast-growing, like diffuse large B-cell lymphoma; needs prompt intervention.